This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
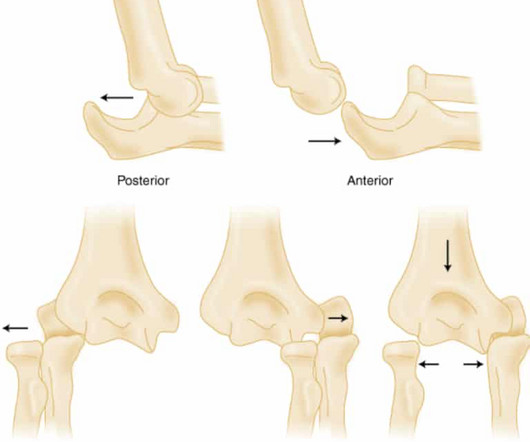
Elbow Dislocation Definition: Disarticulation of the proximal radius & ulna bones from the humerus Epidemiology: Incidence Second most common joint dislocation (after shoulder) in adults Most commonly dislocated joint in children Accounts for 10-25% of all injuries to the elbow ( Cohen 1998 ) Posterolateral is the most common type of dislocation (..)
2013 Mar;34(3):115-24; quiz 125. Jonklaas J, Bianco AC, Bauer AJ, Burman KD, Cappola AR, Celi FS, Cooper DS, Kim BW, Peeters RP, Rosenthal MS, Sawka AM; American Thyroid Association Task Force on Thyroid Hormone Replacement. The patient had no significant past medical history. F); Resp 21; SpO2 99% Constitutional : No distress.
VS abnormalities can drive this as well Strongly consider reversal of AC (this will typically come after control) Stopping the Bleeding PPE: these things bleed like stink. Laryngoscope 2013; 123: 2928-9. Take Home Points: Posterior epistaxis is a rare, life-threatning presentation. Acad Emerg Med 1995; 25(5): 592-6.
Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. It is not yet available, but this is your way to get on the list. link] Case continued She arrived in the ED and here is the first ED ECG.
Etminan 2019) In Belgium between 2010 – 2013, of the 262 children treated with fluroquinolones while hospitalized, only 17% were used for labelled indications. Musculoskeletal Adverse Events include: Articular cartilage damage causing arthralgias or arthritis , Tendonitis , and Tendon rupture. Which is a risk of 1 event for 62.5
mL/kg/hr for 2 consecutive hours OR Decrease in serum lactate by more than 10% from initial level Primary outcome – Early norepinephrine group vs. the control group demonstrated higher rates of shock control at 6 hours: 76.1% vs 48.4% (OR 3.4, vs 48.4% (OR 3.4, vs 48.4% (OR 3.4, of the patients received vasopressors through a peripheral IV.
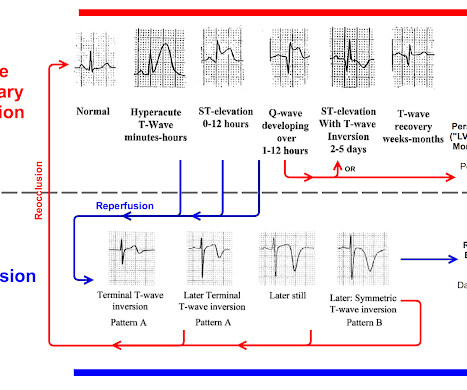
You must understand this and the dynamic nature of ACS to provide excellent care for such patients. Here is the OMI progression of ECG findings for review: You can see that OMI ECG findings must "deflate" and pass through normal or near-normal in order to get to reperfusion findings. This is termed " pseudo-normalization."
Because there was proven thrombus (ACS) but the troponin never went above the 99% reference range (and therefore cannot be called MI -- definition of MI requires rise and/or fall of troponin with at least one value above the 99% reference range), this is UNSTABLE ANGINA with ST Elevation. Fortunately, that is exactly what happened.
This week we’re looking at the other ACS, the surgical ACS, the old abdominal compartment syndrome. This week we’re looking at the other ACS, the surgical ACS, the old abdominal compartment syndrome. These are all very nice and should all be reflected upon and followed when appropriate in your ACS.
Anecdotally, had there been symptoms unequivocally consistent with ACS then one could justifiably make the case for a potential D1 occlusion. Upon arrival he was found alert and oriented, and without gross distress. He denied difficulty breathing, epigastric pain, or chest discomfort. He denied any chest discomfort, or difficulty breathing.
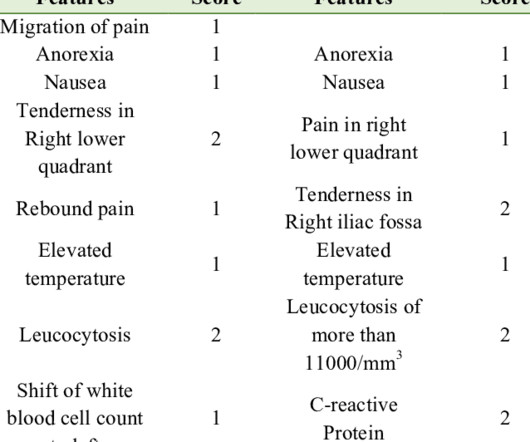
References Meltzer AC, Baumann BM, Chen EH, Shofer FS, Mills AM. 2013 Aug 1;62(2):126-31. Abdominal pain is a common ED presentation and one of the top differential for RLQ pain is Acute Appendicitis. Early in the course, examination findings are often subtle and bloods may not show a raised WCC or CRP. Annals of emergency medicine.
Here is an article I wrote: Updates on the ECG in ACS. Was this: 1) ACS with ischemia and spontaneous reperfusion? Also, anterior MI could result from 1) ACS, but also from 2) severe ischemia due to combination of a hemodynamically significant LAD stenosis + severe hypotension during cardiac arrest. See image with lines below).
Smith: If this is ACS (a big if), t his is just the time when one should NOT use "upstream" dual anti-platelet therapy ("upstream" means in the ED before angiography). History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. Anything more on history?
Although this is considered a "STEMI equivalent" and the ACC/AHA guidelines even approve of thrombolytics for ACS with this ECG, the usual criteria used to alert the cath lab team of an inbound Code STEMI are not met by this ECG. 2 The astute paramedic recognized this possibility and announced a CODE STEMI.
This was formerly an indication for cath lab activation, but was abandoned in the 2013 guidelines because of poor specificity. Here is an algorithm that is very useful in such cases, published by Cai and Sgarbossa in 2013. 1 mm of concordant STE or 2. 1 mm of concordant STD in V1, V2, or V3 3.
2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. The precordial ST-depression pattern on this ECG (and in this clinical setting) should immediately raise suspicion of Posterior STEMI!
Posterior STEMI" may not even technically exist according to the current (2013) ACC/AHA STEMI guidelines, as it is not described as a "STEMI equivalent" and the only relevant statement in the guidelines is: "In addition, ST depression in 2 precordial leads (V1-V4) may indicate transmural posterior injury." J ACC 61(4):e78-140; page e83.
Click here for Direct Download of the Podcast Paper: Aykan AC et al. Because the lungs receive 100% of cardiac output, it has been hypothesized that a lower dose of thrombolytic therapy may still be effective with a better safety profile [3][4]. REBEL Cast Ep123: Reduced-Dose Systemic Peripheral Alteplase in Massive PE?
Since the PREVIEW trial, there have been more negative trials. One such trial was the WASP trial , which involved 477 children in New Zealand. This trial showed no difference in PRAM score or LOS in the prednisolone group compared to placebo. An IPD approach is a collaborative exercise including the authors of included studies and stakeholders.
Notable Physical Exam: General: Tripoding, severe respiratory distress. However, emergency physicians have recently faced a multitude of patients requiring ETI with anatomically and physiologically difficult airways; these patients increase the risk of a can’t intubate/can’t oxygenate scenario or significant hypoxemia, hypercarbia, or acidemia.
But if they do present: The very common presentation of diffuse STD with reciprocal STE in aVR is NOT left main occlusion , though it might be due to sub total LM ACS, but is much more often due to non-ACS conditions, especially demand ischemia. Total LM occlusion can present with STE or STD in aVR. D1 ( STE I, aVL, V5, V6 ) and 2b.
Of note, in the paper by Russotto et al., the patients had to have an oxygen saturation greater than 80%, a blood pressure of 90 SYS/MAP 65 or higher, and not have required intubation due to cardiac arrest prior to the intubation procedure for inclusion. How Do I Predict Physiologically Difficult Airways? Recommendations : 1. are at high risk.
BP gradually rose. She was completely comatose (GCS = 3) and pupils were midposition and fixed. Later in the case there was some respiratory effort but no improvement in pupils or any other aspect of the neurologic exam. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Kurkciyan et al.
8 , 9 The most recent American College of Cardiology and American Heart Association ST-elevation myocardial infarction (STEMI) guidelines (2013) give no direction on diagnosing occlusion myocardial infarction in patients with ventricular paced rhythm. The ED physician attempted to explain the modified Sgarbossa criteria, but without success.
How would an ABG even change the initial stabilization of any of these patients? What alternative testing can be done in these circumstances? Recent studies suggest that clinicians can obtain similarly actionable results from VBGs as ABGs and using the “gold standard” ABG might not be as clinically relevant as it once was.
However, symptoms may also be non-specific, including irritability, headache, poor feeding, vomiting, or diarrhoea. The diagnosis is clinical and can be made by directly visualising erythema or bulging of the tympanic membrane. Treatment is mainly symptomatic with analgesia. A throat culture is the gold standard for confirming a bacterial infection.
saline (NS) solutions are both isotonic crystalloids widely used for intravenous fluid resuscitation across many contexts and disease states ( Myburgh 2013 ). Paper: Alwang AK, Law AC, Klings ES, Cohen RT, Bosch NA. Lactated Ringer (LR) and 0.9% To assess the clinical impact and relevance of these concerns, Alwang et al.
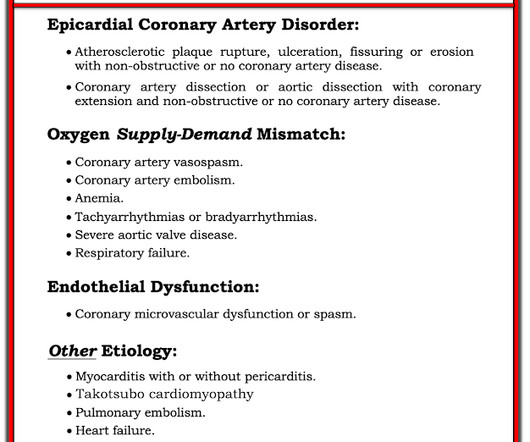
Myocardial Infarction with Non-Obstructive Coronary Arteries. Etiologies (list not comprehensive): Coronary Spasm. Provocative testing is very helpful for this Coronary Thrombus with lysis (one must do optical coherence tomography or at least intravascular ultrasound to find thes non-obstructive plaques that ruptured. Embolism with lysis.
He has a glove and stocking pattern of numbness to his extremities. Motor and sensory findings are symmetrical. Patellar reflexes are 1+. He has no saddle anesthesia or back pain and denies any difficulty urinating or issues with defecation. Paraquat Influenza vaccine Methanol Organophosphate Are his symptoms reversible?
2023 May;182(5):2013-2026 QuantiFERON-TB Gold Plus Performance in Children: A Narrative Review. De Alwis AC, et al. This comprehensive list is developed from 34 journals, including major and subspecialty paediatric journals. N Engl J Med. 2023 May 11;388(19):1755-1766. Mondardini MC, et al. Eur J Pediatr. Buonsenso D, et al.
Left lower lung field end demonstrates expiratory wheezing on auscultation. Other lung fields unremarkable. smoke, high ozone levels, smog) Asthma/reactive airway disease (RAD) Diagnostic criteria 7,8 Respiratory symptoms +/- fever (at least 38.0 C or 100.4 mg/kg, max 4 mg per dose q20-30min) or hydromorphone (0.01-0.02 mg/kg, max 0.4 C or 100.4
Patients with suspected ACS should be evaluated with echocardiography. It will probably show an occlusion of the LAD, and it might be difficult to know how long the occlusion has been there and how viable the myocardium is, but it needs to be opened. Let us have a look at the limb lead ST-T changes. Is this ST elevation ischemic in nature?
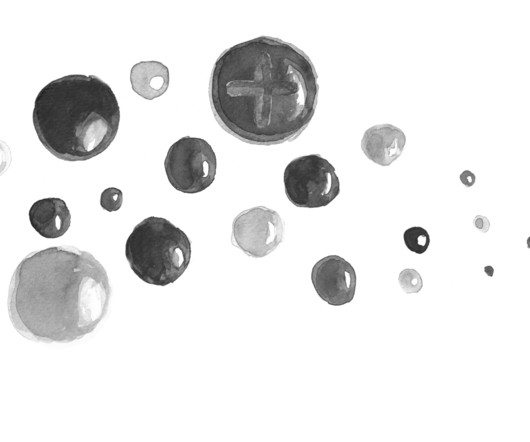
Questions: What is the most likely causative xenobiotic that led to these findings? Influenza vaccine Methanol Organophosphate Paraquat Are her symptoms reversible? Yes No What therapy or therapies are critical for this patient? The exposure can be either intentional or unintentional. 7, 9 Often have absence of excessive cholinergic stimulation.
After completing the ACS algorithm with amiodarone and lidocaine, there are diminishing returns on further treatments. In lab, patients are monitored on continuous abbreviated ECG with 5 electrodes. During ballooning, we often see immediate hyperacute T waves. The patient's ECG at the beginning of the case is shown below. SanzRuiz, R.,
The patient denies any current symptoms but states that he just wants to get checked out. He has no chronic medical conditions, does not take any medications, and does not use any drugs or alcohol. Vital signs are within normal limits, with BP 110/70 mmHg, HR 60 bpm, RR 18 breaths/min, O2 saturation 98% on RA, T 37 C.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.































Let's personalize your content