This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
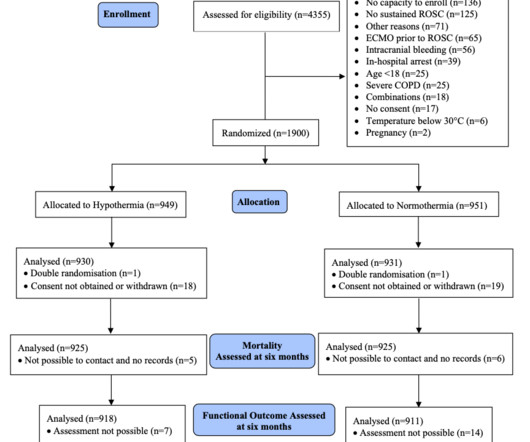
Paramedics managed to get return of spontaneous circulation after a single defibrillation, but the patient is still comatose on arrival. This is the original Target Temperature Management (TTM) trial by Nielson et al NEJM 2013. The charge nurse turns to you and asks: should I grab the ice packs? This gives a NNT of 4.
She was found to be in ventricular fibrillation and was defibrillated 8 times without a single, even transient, conversion out of fibrillation. She was immediately intubated during continued compressions, then underwent a 9th defibrillation, which resulted in an organized rhythm at 42 minutes after initial arrest. It was stented.
The patient received 1 mg of epinephrine IV x2 with conversion of his rhythm to ventricular fibrillation (VF) for which he was defibrillated twice in the field. The patient is moved over to the stretcher and connected to the monitors and defibrillator. What would your next steps be? His point-of-care labs return with a potassium of 3.4
On arrival, vital signs are stable with a HR of 71, BP of 121/71 mmHg, RR of 17 bpm, and SpO2 of 97% on room air. Physical exam reveals a well-appearing female in no acute distress. Cardiac exam is unremarkable with normal S1/S2 without rubs, gallops or murmurs. Neurological exam is also unremarkable. Her presenting EKG is shown below.
She was never seen to be in ventricular fibrillation and was never defibrillated. She was hypotensive in the ED and her bedside echo showed a normal RV and LV. BP gradually rose. She was completely comatose (GCS = 3) and pupils were midposition and fixed. Kurkciyan et al. In 25 (93%), the initial rhythm was asystole or PEA. Results: Over 8.5
Cardioversion/defibrillation. It helps a little bit. Only 5-18% of ED patients with chest pain have a myocardial infarction of any kind. Only 1-5% have OMI. Anyone with a baseline Brugada pattern ECG can have esophageal pain, or chest wall pain, and then be thought to be having an MI based upon a false positive ECG. How can this be 'Not MI'
Schick is a PGY3 at the Brown Emergency Medicine Residency in Rhode Island. I remember Allie well from her days in the Research volunteer program at Hennepin. The article is edited by Smith. Title: Is it just hot in here or is it a OMI? See additional image at the bottom of this post. Could this be induced by elevated core temperature? F (rectal).
We rapidly defibrillated her, and with return of normal sinus rhythm. Several minutes later the patient developed V-fib again > 200J defibrillation with return to NSR. Rapid sequence intubation was performed for airway protection in setting of recurrent V-fib and defibrillations. Chest X-ray also showed pulmonary edema.
Several 200 J shocks did not terminate the VF, so a second defibrillator was applied for double sequential defibrillation with 400 J. She was defibrillated perhaps 25 times. In lab, patients are monitored on continuous abbreviated ECG with 5 electrodes. During ballooning, we often see immediate hyperacute T waves.
He was defibrillated twice and received two doses of epinephrine, with return of spontaneous circulation. He underwent placement of a dual chamber, implantable, cardioverter-defibrillator (ICD) placement on hospital day 5. There was no family history of syncope or sudden death. Figure 1: The EMS rhythm strip.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















Let's personalize your content