This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Do we need to intubate French drunkards in ED? 2013 Sep;24(9):1848-53. Epub 2013 Jul 17. Justin and I discuss 7 papers covering a range of topics from securing IVCs in kids to intubating in space and the use of religious sham artifacts in middle-age, French “psychiatry” Yep, it was a strange month on the pod!
1 History and physical examination have been the cornerstone of seizure diagnosis in the emergency department (ED). 2 A study of routine EEG in the ED in 2013 found that five percent of ED patients with altered mental status had nonconvulsive seizures (of whom 75 percent were in nonconvulsive status epilepticus).
Background: The immediate post intubation period in the ED is a critical time for continued patient stabilization. The reality of ever increasing ED volumes and longer boarding times to the ICU makes it imperative for emergency physicians to learn how to manage these critical patients. mg/kg over several minutes 0.02 – 0.1
fold higher risk of NSTI than the control group 12 For those without comorbidities , AUD exhibited a 15.2-fold fold higher risk of NSTI than the control group 12 For those without comorbidities , AUD exhibited a 15.2-fold fold higher risk of NSTI than the control group 12 For those without comorbidities , AUD exhibited a 15.2-fold
However, RSI has never been shown to reduce the risk of aspiration in the ED (13) or during emergent OR cases (14). While RSI should remain the gold standard in the vast majority of patients in the ED, FI presents an additional technique to mitigate anatomic or physiologic risk. To date, ketamine has been the agent of choice (12).
More than 1/3 of geriatric trauma patients presenting to the ED after a fall return to the ED or die within one year of initial evaluation. 4 Elderly patients, who comprise only 8-12% of total ED major trauma cases, represent a disproportionate 15-30% of trauma mortalities and costs. Int J Emerg Med 2013; 6:12.
Louis) // Reviewed by: Alex Koyfman, MD (@EMHighAK); Brit Long, MD (@long_brit) Case You are working in the trauma/critical care pod of your emergency department (ED). His blood sugar was normal en route to the ED, and his initial rhythm on the cardiac monitor was asystole. 2013 Jan 24;368(4):394]. Resuscitation. N Engl J Med.
You, however, are working an ED shift, and when you see the name “Barbie Junior” on your computer screen, your heart does a flutter. It can be in started in the ED, and many of us are already using it. Secondary outcome analysis showed there was no difference in length of hospital stay, ICU stay, or duration of oxygen therapy.
Submitted and written by Destiny Folk MD , peer reviewed by Meyers, Smith, Grauer, McLaren A man in his early 30s with no significant past medical history was brought to the ED by EMS after being found unresponsive by a friend. On arrival in the ED, he was hypotensive with a systolic blood pressure in the 70s.
As the only respiratory therapist in the ED has been paged and is starting BiPAP for this patient, an overhead call for two incoming trauma alerts from a multivehicle collision sounds. Because the RT responsible for drawing arterial blood gases is busy caring for these patients, ABGs will be delayed.
4,11 Oral corticosteroids are as effective as intravenous steroids, but a one-time dose of intravenous methylprednisolone 125 mg in the ED is useful for patients who obviously cannot tolerate oral medications. Tintinalli JE, Stapczynski JS, Ma OJ, et al, eds. 1 Titrate to oxygen saturation of 88-92 percent. 5 mg plus ipratropium 0.5
saline (NS) solutions are both isotonic crystalloids widely used for intravenous fluid resuscitation across many contexts and disease states ( Myburgh 2013 ). Applicability to Emergency Medicine: For emergency medicine providers, the greatest challenge with this study is that it did not include or account for ED care.
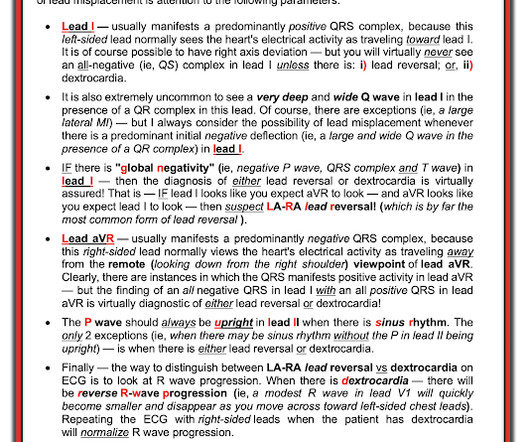
On arrival in the ED, a bedside ultrasound showed poor LV function (as predicted by the Queen of Hearts) with diffuse B-lines. Smith insightfully noted on seeing the initial ED ECG in today's case, "This is very bad.". For clarity in Figure-1 I've reproduced and labeled this initial ED ECG.
Sepsis There has been much controversy over the last two decades around the various nuances of volume resuscitation in ED patients with suspected sepsis, much of which goes beyond the scope of this limited review. For links to FOAM-ED ultrasound content, see the section after take-home points.) In 2013 Richer et al.
An 8-year old male with a history of sickle cell anemia presents to the ED for evaluation of fever for 2 days and “feeling like I can’t get a full breath”. 768: Epidemiology of Hospital Based ED Visits due to Sickle Cell Crisis and Acute Chest Syndrome in Kids. Critical Care Medicine 41(12):p A191, December 2013. PMID: 29648482.
Today, increased mortality rates, higher transfusion requirements, and lengthened ICU stays are recognized as proximate effects of the Trauma Triad. upon ED arrival incur mortality rates of up to 3-5x that of patients without coagulopathy. 2013 Apr 17;10(6):747-50. Current literature suggests that patients with INR > 1.2
F, HR 48, RR 28, BP 104/62, SPO2 88% on non-rebreather mask The patient’s friend who brought her to the ED tells you the patient made suicidal statements earlier in the day and was found in her yard shed. These are send-out labs with turn-around times that make them unlikely to affect the ED course or guide treatment. 2013; 6:524.
doi: 10.1136/emermed-2013-202449. Epub 2013 Jul 14. but PPV ranges from 25.1-39.5% years Internal validation cohort: 43,400 patients with mean age 3.7 years External validation cohort: 45,855 patients with mean age 2.6 0.38 (95% CI 0.20-0.39) 0.39) AUROC of 0.71-0.92 0.92 (95% CI 0.70-0.92) and PPV of 5.3-7.1% and PPV of 22.2%
While this guide isnt exhaustive, its designed by residents, for residents, to provide practical tips and foundational knowledge thats crucial in the fast-paced, high-stakes environment of the ED. Introduction Airway management is a critical ED skill to master. Figure 4 : Demonstration of Mallampati classes.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content