This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The ECG is just a test: a Bayesian approach to acute coronary occlusion If a patient with a recent femur fracture has sudden onset of pleuritic chest pain, shortness of breath, and hemoptysis, the D-dimer doesn’t matter: the patient’s pre-test likelihood for PE is so high that they need a CT. Circulation 2014 2. But does this matter?
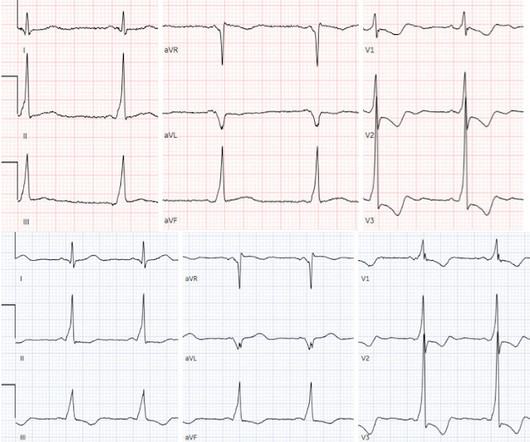
Note that as many as 7% of patients with acute coronary syndrome have chest pain reproducible on palpation [Lee, Solomon]. which reduces the pre-test probability of acute coronary syndrome by less than 30% [McGee]. The note also says "slight lateral ST elevations noted, likely early repolarization since unchanged compared to 2014."
Smith: If this is ACS (a big if), t his is just the time when one should NOT use "upstream" dual anti-platelet therapy ("upstream" means in the ED before angiography). History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. Anything more on history?
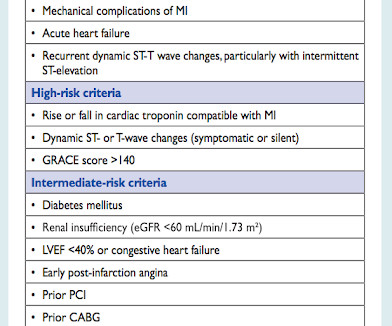
We could not rule out acute epicardial coronary (large artery) occlusion. Learning Point Acute coronary occlusion may occur with no ECG findings whatsoever. This is from the 2014 ACC/AHA guidelines. Patients with ACS and hemodynamic instability 2. Patients with ACS and acute pulmonary edema 3. This includes: 1.
The diagnostic coronary angiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aortic valve. Author continued : STE in aVR is often due to left main coronary artery obstruction (OR 4.72), and is associated with in-hospital cardiovascular mortality (OR 5.58).
Other possible reasons for higher levels could be: Pregnancy Coronary Artery Disease Viral Infections (10–40 mg/L) Bacterial infection (>40mg/dL) Malignancy, Obstructive Sleep Apnea, Connective Tissue Disorders Serial CRP measurements may be helpful to monitor a patient’s response to medical intervention. 2014 Jan 1;3(1):1-5.
The AHA/ACC guidelines recommend emergent cardiac catheterization for patients with concern for ACS and refractory chest pain despite maximum medical therapy defined as aspirin + clopidogrel/ticagrelor + heparin/enoxaparin. link] He was admitted to the cardiology unit for serial troponin measurements and concern for possible ACS.
A 68-year-old male with a past medical history of hypertension, diabetes mellitus, and coronary artery disease with a drug eluting stent placed 2 months ago presents with dizziness and vomiting that began 3 hours ago. The NIHSS cutoff that predicts outcomes is 4 points higher in AC compared with PC infarctions. Epub 2014 Dec 4.
It was a 60yo with a history of stents to the circumflex and right coronary arteries, who presented with 9 hours of fluctuating central chest pain. This is step 4 : relying on the first troponin level to rule out acute coronary occlusion. 4] CT revealed no dissection but extensive coronary atherosclerosis.
The emergency physician wasn’t sure what to make of the changes from one ECG to the next but was concerned about ACS. CMAJ 2014. Int J Cardiol 2014. == MY Comment by K EN G RAUER, MD ( 10/13/2022 ): == I suspect most cases of acute OMI that occur in association with WPW — are overlooked! What do you think? Chang and Liu.
For the same reason, you should not delay coronary angiography because pain resolves with morphine. Both the outdated 2014 AHA/ACC guidelines and the updated 2023 ESC guidelines recommend immediate invasive management of patients with uncontrolled chest pain. 2023 ESC guidelines for the management of acute coronary syndromes.
Background: Historically, we have treated acute coronary syndrome with supplemental oxygen regardless of the patient ’ s oxygen saturation. More recent evidence, however, demonstrates that too much oxygen could be harmful ( AVOID Trial ) by causing coronary vasoconstriction and increasing oxidative stress. Low O2 protocol: 3.1%
A 94-year-old female with a past medical history of hypertension, coronary artery disease, chronic venous stasis, and permanent pacemaker placement initially presented to triage complaining of left hip pain in the setting of a fall shortly prior to arrival. doi: 10.21037/acs.2016.05.04. 2014 Jul; 3(4):351-67. 2016 May; 5(3):256.
Click here for Direct Download of the Podcast Paper: Aykan AC et al. PMID: 23102885 Aykan AC et al. Because the lungs receive 100% of cardiac output, it has been hypothesized that a lower dose of thrombolytic therapy may still be effective with a better safety profile [3][4]. Clin Exp Emerg Med 2023. CHEST 2010. Am J Cardiol 2013.
The patient would not have been diagnosed with acute coronary syndrome and would not have had an angiogram, would have been discharged (or perhaps had a stress test, which would be negative), and would be at great risk of another event, possibly resulting in death or heart failure. Imagine if you had only recorded the 2nd ECG. Thelin et al.
Below follows a drug manual for use in the CCU (coronary care unit), ICU (intensive care unit) or ER (emergency room). μg/kg/min + + + ++ Low dose dopamine stimulates D1 receptors and induces vasodilation in coronary, renal, cerebral and mesenteric vessels. Increases coronary blood flow. Coronary flow enhanced.
She did not receive any opioids (which would mask her pain without affecting any underlying ACS). The Portable Programmable Microprocessor-Driven Real-Time 12-Lead Electrocardiographic Monitor: A Preliminary Report of a New Device for the Noninvasive Detection of Successful Reperfusion or Silent Coronary Reocclusion. Meisel et al.
You review his chart and note that he had a heart transplant in 2014 but has not followed up with a cardiologist for at least 3 years. 3,10 Coronary Allograft Vasculopathy Nicknamed “The Achilles Heel of Heart Transplantation,” this accounts for the majority of patient mortality in the 5-10 year range.
54 It is vital to consider dangerous epigastric pain mimickers like acute coronary syndrome (ACS), hepatobiliary disease, or pancreatitis. doi:10.1136/heartjnl-2014-306362 LeWinter MM. Comparison of factors associated with atypical symptoms in younger and older patients with acute coronary syndromes. doi:10.1097/SPC.0000000000000437
The arterial pressure waveform is transduced using the coronary catheter. Normally, the diameter of the coronary artery ostium is much greater than the diameter of the catheter so that catheter engagement does not significantly impair antegrade coronary perfusion. Here is the ECG and arterial waveform during RCA angiography.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

























Let's personalize your content