This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
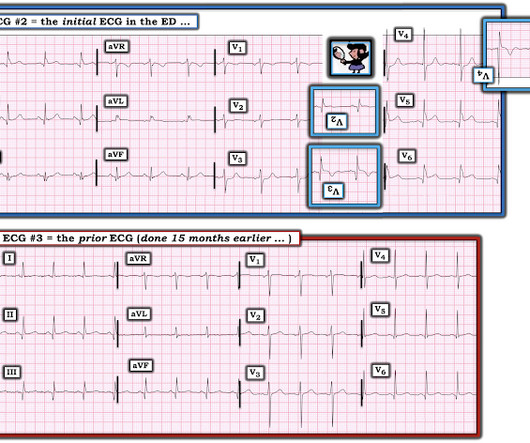
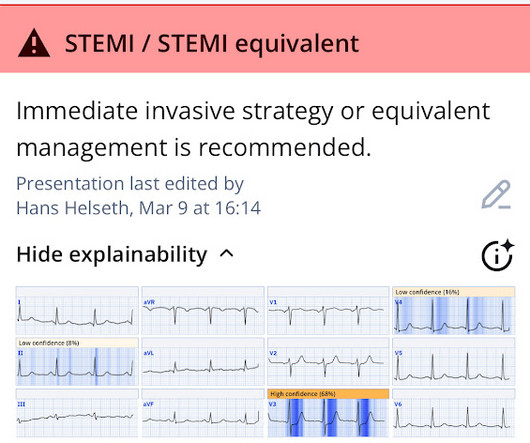
Note that as many as 7% of patients with acute coronary syndrome have chest pain reproducible on palpation [Lee, Solomon]. which reduces the pre-test probability of acute coronary syndrome by less than 30% [McGee]. The note also says "slight lateral ST elevations noted, likely early repolarization since unchanged compared to 2014."
Studies have shown that oxygen can cause vasoconstriction, increase blood pressure and decrease coronary artery blood flow ( Kones et al AM J Med 2011). Oxygen supplementation in non-hypoxemic patients with acute myocardial infarction has been a hot topic since the publication of the AVOID-trial ( Stub et al Circulation 2014).
The ECG is just a test: a Bayesian approach to acute coronary occlusion If a patient with a recent femur fracture has sudden onset of pleuritic chest pain, shortness of breath, and hemoptysis, the D-dimer doesn’t matter: the patient’s pre-test likelihood for PE is so high that they need a CT. But does this matter?
For the same reason, you should not delay coronary angiography because pain resolves with morphine. Both the outdated 2014 AHA/ACC guidelines and the updated 2023 ESC guidelines recommend immediate invasive management of patients with uncontrolled chest pain. So I would be worried about inferior OMI. At midnight.
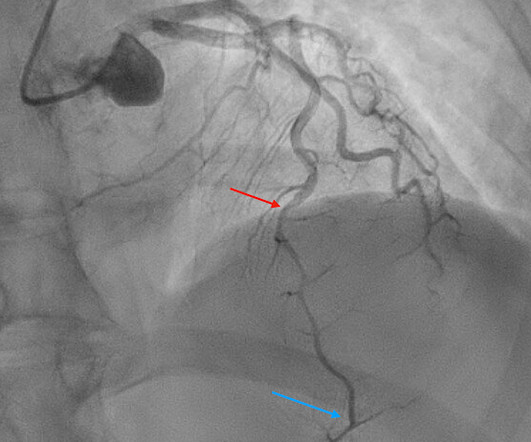
I quickly reviewed the patient’s records and saw that she was a 53 year old woman with a history of BMI 40, but no other identifiable risk factors for coronary artery disease. In this patient with stuttering symptoms and rising troponin, there is no other option but to perform emergent coronary angiography. Hers is shown below.
Thanks in part to rapid bedside diagnosis, the patient was able to avoid emergent coronary angiography. Consider the following: We become attuned to looking for acute coronary occlusion in patients who present with acute symptoms to the ED ( E mergency D epartment ). What do you do clinically when the ECG looks like this?
Background: Historically, we have treated acute coronary syndrome with supplemental oxygen regardless of the patient ’ s oxygen saturation. More recent evidence, however, demonstrates that too much oxygen could be harmful ( AVOID Trial ) by causing coronary vasoconstriction and increasing oxidative stress. Low O2 protocol: 3.1%
in the paper but 2.7% to ≈0.99 (p<0.001) Mean MPI/Tei Index≈ 0.47 in the paper but 2.7% to ≈0.99 (p<0.001) Mean MPI/Tei Index≈ 0.47 in the paper but 2.7% to ≈0.99 (p<0.001) Mean MPI/Tei Index≈ 0.47 to 4.0mg/hr typically given in EKOS therapy (See Below).
GLP-1 agonists are also associated with improved ejection fraction, coronary blood flow, and cardiac output while reducing the risk of cardiovascular events, infarction size, and all-cause mortality. The effects of GLP-1 agonists are associated with the dose. Higher doses of GLP-1 agonists are associated with weight loss.
Video 3: Coronary approach to the gallbladder POCUS Findings Sonographically, the gallbladder is situated in the right upper quadrant as an elongated pear-shaped organ on the inferior surface of the liver. New York, NY: The McGraw-Hill Companies; 2014. Often, you will see bowel gas, which is an indication you are too inferior.
A 68-year-old male with a past medical history of hypertension, diabetes mellitus, and coronary artery disease with a drug eluting stent placed 2 months ago presents with dizziness and vomiting that began 3 hours ago. We’ll keep it short, while you keep that EM brain sharp. Symptoms may range from days to months prior to stroke onset.
Hgb 11g/dL (110g/L) and leukocytosis, and a mildly elevated troponin (36 ng/L, with normal 1mm STE in aVR due to ACS will require coronary artery bypass surgery for revascularization, the infarct artery is often not the LM, but rather the LAD or severe 3-vessel disease. Incidence of an acute coronary occlusion. link] Harhash AA et al.
We could not rule out acute epicardial coronary (large artery) occlusion. Learning Point Acute coronary occlusion may occur with no ECG findings whatsoever. It was not relieved by anything. The pain was not positional, pleuritic, or reproducible. He had no previous medical history. The blood pressure was 110/60. mm STE in one lead.
Coronaries were normal, as was serial troponin. Written by Jesse McLaren Two patients in their 70s presented to the ED with chest pain and RBBB. Do either, both, or neither have occlusion MI? Patient 1 : a 75 year old called paramedics with one day of left shoulder pain which migrated to the central chest, which was worse with deep breaths.
The diagnostic coronary angiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aortic valve. Author continued : STE in aVR is often due to left main coronary artery obstruction (OR 4.72), and is associated with in-hospital cardiovascular mortality (OR 5.58).
It was a 60yo with a history of stents to the circumflex and right coronary arteries, who presented with 9 hours of fluctuating central chest pain. This is step 4 : relying on the first troponin level to rule out acute coronary occlusion. 4] CT revealed no dissection but extensive coronary atherosclerosis.
The patient proceeded to cath where all coronaries were described as normal with no evidence of any CAD, spasm, or any other abnormality. Written by Pendell Meyers A man in his 70s with no cardiac history presented with acute weakness, syncope, and fever. He denied chest pain or shortness of breath. PM Cardio digitized version.
WPW, previous Q wave MI, and acute coronary occlusion Depending on the location of the accessory pathway, WPW pattern can mimic ventricular hypertrophy (including RVH or LVH) or myocardial infarction (including anterior, inferior, lateral or posterior MI) [1]. See these 5 cases of WPW mimicking and/or obscuring acute OMI Take home 1.
I want all to know that, with the right mind preparation, and the use of the early repol/LAD occlusion formula, extremely subtle coronary occlusion can be detected prospectively, with no other information than the ECG. It is not a missed STEMI, but it is a missed coronary occlusion. Wang T, Zhang M, Fu Y, et al. Marti D et al.
Emergent CT coronary angio also likely has a role in such cases. Like they would for any other acute arterial occlusion syndrome (such as suspicion of acute large vessel stroke), they take the patient across the hall and perform an immediate CT (coronary) angiogram, showing patent coronaries. I immediately responded: "cool fake!
Other possible reasons for higher levels could be: Pregnancy Coronary Artery Disease Viral Infections (10–40 mg/L) Bacterial infection (>40mg/dL) Malignancy, Obstructive Sleep Apnea, Connective Tissue Disorders Serial CRP measurements may be helpful to monitor a patient’s response to medical intervention. 2014 Jan 1;3(1):1-5.
Below follows a drug manual for use in the CCU (coronary care unit), ICU (intensive care unit) or ER (emergency room). μg/kg/min + + + ++ Low dose dopamine stimulates D1 receptors and induces vasodilation in coronary, renal, cerebral and mesenteric vessels. Increases coronary blood flow. Coronary flow enhanced.
Open angle Closed angle Definitions Increased resistance to aqueous outflow through the trabecular meshwork. Most common type of glaucoma Occurs with obstruction to aqueous outflow, usually from the iris. Most common cause: pupillary block. Symptoms Generally painless, asymptomatic. May have blurred vision or decreased visual acuity.
The patient would not have been diagnosed with acute coronary syndrome and would not have had an angiogram, would have been discharged (or perhaps had a stress test, which would be negative), and would be at great risk of another event, possibly resulting in death or heart failure. Suppose you had used the formula? Thelin et al.
Identifying patients with low risk for acute coronary syndrome without troponin testing: validation of the HEAR score. High-sensitivity cardiac troponin I at presentation in patients with suspected acute coronary syndrome: a cohort study. Case Rep Emerg Med 2014 7. Backus BE, Six AJ, Kelder JC, et al. Int J Cardiol 2013 2.
Despite having acute coronary occlusion by cath, his ECGs never met STEMI criteria. However, even if there hadn't been exclusion criteria present on this ECG (QRS distortion), these formulas are not perfectly sensitive or specific even in the derivation studies (around 90%). Teaching points: 1.
This is most consistent with ischemia/infarction in the distribution of the left circumflex coronary artery. Figure-1: Illustration of the rational for the Mirror Test ( Figure excerpted from Grauer K: ECG-2014 Pocket Brain ePub ). Regional wall motion abnormality-inferior base ( this is the posterior wall ). What is the “Mirror” Test?
1 The primary goal of cardiopulmonary resuscitation (CPR) is to optimize coronary perfusion pressure and maintain systemic perfusion in order to prevent neurologic and other end-organ damage while working to achieve ROSC. Interventions during the acute phase of treatment post return of spontaneous circulation (ROSC) are therefore critical.
The Portable Programmable Microprocessor-Driven Real-Time 12-Lead Electrocardiographic Monitor: A Preliminary Report of a New Device for the Noninvasive Detection of Successful Reperfusion or Silent Coronary Reocclusion. Echo showed anterior septal, anterior wall, and apical wall motion abnormalities, as well as an EF of 45%. Patel et al.,
A 94-year-old female with a past medical history of hypertension, coronary artery disease, chronic venous stasis, and permanent pacemaker placement initially presented to triage complaining of left hip pain in the setting of a fall shortly prior to arrival. 2014 Jul; 3(4):351-67. Neuro : Awake, alert, oriented x 3. g/dL, 41.5%
You review his chart and note that he had a heart transplant in 2014 but has not followed up with a cardiologist for at least 3 years. 3,10 Coronary Allograft Vasculopathy Nicknamed “The Achilles Heel of Heart Transplantation,” this accounts for the majority of patient mortality in the 5-10 year range.
of very high risk NSTEMI patients underwent angiography in less than 2 hours in accordance with the 2014 ACC/AHA guidelines. Immediate and early percutaneous coronary intervention in very high risk and high risk non-ST segment elevation myocardial infarction patients. Lupu et al. Clinical Cardiology. Am Heart J [Internet].
He also reports associated photophobia, nausea, and a single episode of vomiting in the lobby. He denies a history of similar headaches in the past. He denies any medical history, significant family history, or recreational drug use. Vital signs: Temperature 99.5F, HR 98 bpm, BP 162/86 mmHg, RR 14 per minute, oxygen saturation 99% on room air.
The pain is worse with deep breaths, coughing, or certain movements, and improves with rest and nonsteroidal anti-inflammatory drugs (NSAIDs). A 45-year-old male presents to the ED after a motor vehicle collision where he was the restrained driver. He reports severe, localized chest pain, worsened by breathing, coughing, and movement.
The arterial pressure waveform is transduced using the coronary catheter. Normally, the diameter of the coronary artery ostium is much greater than the diameter of the catheter so that catheter engagement does not significantly impair antegrade coronary perfusion. During ballooning, we often see immediate hyperacute T waves.
Heitner et al found that in 14% of patients with NSTEMI, a blinded interventional cardiologist interpreting coronary angiograms identified a different culprit artery than CMR ( [link] ). Meanwhile acute coronary occlusion causing an isolated posterior OMI was not recognized by several providers, including the consulting cardiologist.
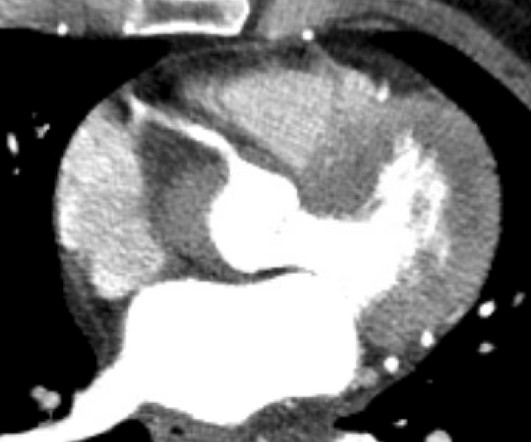
Cardiology wanted a CT of the aorta to rule out dissection, presumably partly due to the very high blood pressure readings, but also because it is hard for people to believe that a 20-something woman could have acute thrombotic coronary artery. They also recommended a NTG drip, after which she reported complete resolution of pain. Denies SOB.
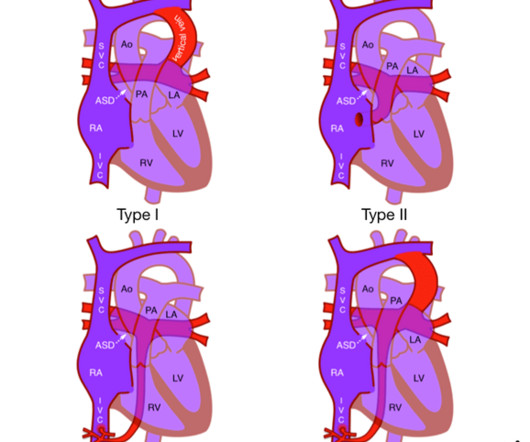
Cardiac TAPVD (25%) : Drainage is directly to the right atrium, typically via the coronary sinus. This usual anatomical arrangement is found in 6070% of people. 2 Anatomy in TAPVD In TAPVD, all four pulmonary veins (PV) have abnormal connections, either to the systemic veins, the right atrium (RA), or both. 3 How do we diagnose TAPVD?
There are currently three methods available for combined hormonal contraception: combined oral contraceptive pills transdermal patch vaginal ring Oral Contraceptive Pills The pill is taken every day for three weeks (or for longer in an extended pill pack), and then either a placebo or low-dose pill is taken for one week to allow menstruation.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content