This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Case: A 37-year-old man without a significant past medical history presents to the emergency department (ED) with a chief complaint of lower back pain that started three days prior to the ED visit after unloading a truck with furniture. His twitter handle is @PainFreeED.
A quick primer on hypocalcemia in the ED. Pfenning CL, Slovis CM: Electrolyte Disorders; in Marx JA, Hockberger RS, Walls RM, et al (eds): Rosen’s Emergency Medicine: Concepts and Clinical Practice, ed 8. 2014, (Ch) 125: p 1636-53. Diagnosis and management of hypocalcaemia. BMJ 2008; 336:1298. Louis, Mosby, Inc.,
The current outbreak of the novel respiratory pathogen Coronavirus is an opportunity to remind ourselves of how to properly and adequately prepare for an emergency outbreak in our EDs. The post Preparation for Emergency Infectious Outbreak in your ED – Coronavirus appeared first on Emergency Medicine Cases.
fold higher risk of NSTI than the control group 12 For those without comorbidities , AUD exhibited a 15.2-fold fold higher risk of NSTI than the control group 12 For those without comorbidities , AUD exhibited a 15.2-fold fold higher risk of NSTI than the control group 12 For those without comorbidities , AUD exhibited a 15.2-fold
Case: A 24-year-old manual labourer presents to the emergency department (ED) after drinking a few too many beers, having a disagreement with another beer drinker and gets knocked down. Background: Fractures of the scaphoid are the most common carpal fractures presenting to the ED. We went into some detail on SGEM#385.
It is commonly missed during the first few ED visits. Keep a high index of suspicion for anti-NMDAr encephalitis in children and adolescents who have had multiple ED visits for new and worsening psych/behavioral concerns, seizures, and/or movement disorders over several months. 2014 Feb;13(2):167-77. 2014 Feb;13(2):135.
Case: You are doing great things and helping many patients during your shift in the emergency department (ED) when you hear a trauma alert being called overheard. A clinical decision tool called the STUMBL score was derived and validated by Battle et al in 2014 [3]. These risks are particularly higher in the elderly [2].
Case: A 5-year-old boy presents to the emergency department (ED) with his parents for fever and fatigue. Background: We have looked at pediatric vital signs on the SGEM back in 2014 with PedEM superhero Dr. Anthony Crocco ( SGEM#98 ). He has had three days of high fevers at home. It seems awfully high. Does he have sepsis?”
In many emergency departments (ED), US machines are readily available and can be used to rapidly assess and monitor patients with acute dyspnea at the bedside. US, compared with CXR and CT, offers the absence of ionizing radiation and high reproducibility. Emerg Med J. 2023;40(10):700-707.
Up to 1/3 of adults over 60 suffer from chronic constipation. Evaluation: A good history and a high index of clinical suspicion is paramount, especially in high-risk patient populations 4 CT of the abdomen and pelvis with contrast is the best choice for diagnosis. Enemas (some studies show this may be associated with perforation risk).
Cardiology consult note written around that time documents that "Pain improved with NTG, morphine in ED but still present." The note also says "slight lateral ST elevations noted, likely early repolarization since unchanged compared to 2014." This patient was not one of the lucky 6.4%
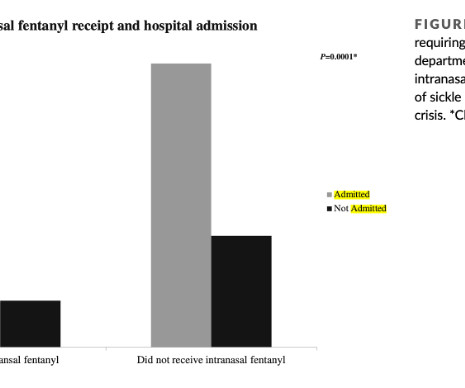
Case: A 14-year-old male with sickle cell disease (SCD) presents to your emergency department (ED) with a vaso-occlusive pain episode (VOE) of his bilateral legs and back. 1-6] Children with SCD presenting to the ED with VOE require timely and effective pain control. He denies any fever or difficulty breathing.
Even though sedation after endotracheal intubation (ETI) reduces the risk of self-extubation, uncontrolled pain, and awakening awareness, several small single-centre studies demonstrate low rates of sedative drug administration after ETI in the emergency department (ED). What are the only exceptions? How can we prevent this?
A 5-year-old female presented to the emergency department (ED) with a one-year history of gradually increasing anterior neck swelling. She was discharged from the ED on levothyroxine 25 mcg daily with endocrinology outpatient follow-up. 2014 Dec;24(12):1670-751. The patient had no significant past medical history.
Author: Natalie Bertrand, MD Editor: Naillid Felipe, MD Background: Definition: adverse reaction to blood product administration Incidence: more common in children than adults, except for delayed hemolytic transfusion reactions Allergic (non-anaphylaxis) – Platelets 1-3%; RBCs 0.1-0.3% mg IF requiring IM Epi >3x, switch to IV Epi, 0.05-0.1
Case: A 45-year-old man without a significant past medical history presents to your emergency department (ED) with two days of severe lower back pain after shoveling some dirt. EDs annually (1). The pain is 10/10 in intensity, gets worse with bending, turning, and prolonged walking. million visits to U.S.
Major takeaway: Consider SBP in any patient who comes into the ED with ascites. Literature concerning risk with PPIs is controversial. Presentation: Classic presentation is abdominal pain or tenderness, fever, and altered mental status. Literature suggests 10-33% of patients are asymptomatic or only have mild symptoms. increase in mortality.
Case: You are in discussion with your emergency department (ED) manager about the number of patients boarding for hours to days and you are both aware that many of these patients are attending with mental health crises. ED visits in the US for mental health conditions has increased by 44% from 2006 to 2014.
The pain is intermittent, sharp, severe, and associated with 2 episodes of nonbloody, nonbilious emesis. Her mother denies any fevers, upper respiratory symptoms, sore throat, or diarrhea. She adds that her daughter has complained of 2-3 episodes of dysuria and gross hematuria over the last few days. Lay the patient supine when possible.
Disulfiram-like reaction with ethanol consumption Coprinus atramentarius or Ink Cap mushroom is well known to cause a disulfiram-like reaction when it is consumed prior to ethanol. This results in significant nausea and vomiting and can lead to tachycardia and hypotension. Read More in the Series References Peredy. Mushrooms, Coprine. Goldfrank L.
In: Nelson LS, Goldfrank LR et al (eds): Goldfrank’s Toxicologic Emergencies. Intensive Care Med 2014; 40(1):104. PMID As ferrioxamine is excreted, the patient’s urine becomes an orange or brown rusty hue, classically referred to as vin rosé urine [1,2]. For iron toxicity, what are the indications for deferoxamine?
A 29-year-old female with a past medical history of migraine headaches presented to the emergency department (ED) for several hours of bilateral eye pain, redness, and decreased visual acuity. Contact Lens Wearer Demographics and Risk Behaviors for Contact Lens-Related Eye Infections–United States, 2014.
However, RSI has never been shown to reduce the risk of aspiration in the ED (13) or during emergent OR cases (14). While RSI should remain the gold standard in the vast majority of patients in the ED, FI presents an additional technique to mitigate anatomic or physiologic risk.
You wonder if any emergency department (ED)-based interventions would help her and people like her be safe. Back then we found that at one academic site older adults attending ED with falls didn’t receive guideline-based assessment, risk stratification or management. There are three other GEAR 1.0 Reference: Hammouda et al.
Case: A 41-year-old man without a significant past medical history presents to the emergency department (ED) with a chief complaint of lower back pain that started 48 hours prior to the ED visits after attempting to move a couch in his house. Background: Pain is one of the most frequent reasons to attend an ED.
SGEM#71 : Like a Rolling Kidney Stone (A Systematic Review of Renal Colic) * Bottom Line: Tamsulosin is useless in most ED patients with ureteral colic unless their stone size exceeds at least 4mm. *
Intranasal Fentanyl for Sickle Cell Vaso-Occlusive Pain Case A 15-year-old female with sickle cell disease (SCD) presents to your emergency department (ED) with a vaso-occlusive pain episode (VOE) of her legs and back. Children with SCD often present to the ED in pain due to VOE. She has a history of similar episodes. Am J Hematol.
Case: A 71-year-old man is brought to your emergency department (ED) by emergency medical serviced (EMS) having fallen two steps at home. Falling is the most common cause of traumatic injury resulting in older adults presenting to the ED [4]. years ( 2 ). years ( 2 ).
Bottom Line Up Top: In patients with infectious processes that are stable for discharge home, there is no role for giving a first dose of antibiotics IV in the ED. Clinical Scenario: A 45-year-old woman with hypertension presents with a productive cough and fever. Her vitals are: HR 115, BP 120/80, Temp 102.8, O2 Sat 99% on RA, RR 18.
Rate Versus Rhythm in the ED The 2023 AHA/ACC guideline doesn’t give explicit recommendations or preference regarding initial rate or rhythm control strategy for new-onset AF patients who are hemodynamically stable. based care of ED patients with AFRVR. The AHA/ACC cites a meta-analysis including five RCTs of 745 participants.
Published 2014 Mar 26. Like opioid intoxication, xylazine exposure may result in [4]: Respiratory depression Bradycardia Miosis Hypotension CNS depression Skin findings from chronic use range from superficial ulcerations and cellulitis to severe soft tissue destruction either at or distant from the IV injection sites. Forensic Sci Int.
A 37-year-old G5P4 at 33 weeks presents to the ED after being brought in by ambulance. We’ll keep it short, while you keep that EM brain sharp. She had a precipitous delivery while the ambulance was pulling in. The newborn is doing well, but the mother is complaining of shortness of breath and chest pain.
Oxygen supplementation in non-hypoxemic patients with acute myocardial infarction has been a hot topic since the publication of the AVOID-trial ( Stub et al Circulation 2014). However, this difference between the two groups was not statistically significant (relative risk 0.9; What would you rather have, more death or less VT?
The risk of a biphasic reaction is what keeps patients in the ED while being observed for a set period of time. up to 23% ( Lieberman 2005 , Rohacek 2014 , Tole 2007 , Grunau 2014 ). Since half of biphasic reactions occur within the first 6-12 hrs ( Lee 2014 ) physicians often choose an observation time of 4-6 hrs.
Here’s another case from Medical Malpractice Insights – Learning from Lawsuits , a monthly email newsletter for ED physicians. In 2014 I was asked by 4 different plaintiff attorneys to review 4 separate cases of a missed SEA, all in Washington State. To opt in to the free subscriber list, click here. It’s a simple 3 step process: 1.
Philadelphia: Elsevier Saunders; 2014:805-807. Possible early antibiotic treatment Minor Marine Trauma Mechanism: Bites, Stings, Nematocysts Envenomation Presentation: All can cause localized pain, erythema, and warmth Dermatologic: Urticaria, burning, pruritus, localized paresthesia. Marine Trauma and Envenomation. Accessed August 25, 2022.
PMID: 34697777 Clinical Question: In patients with moderate to severe alcohol withdrawal being discharged from the emergency department (ED), does treatment with phenobarbital alone and phenobarbital plus benzodiazepines compared to benzodiazepines alone decrease the odds of returning to the ED within 3 days after initial discharge?
Patient is asymptomatic. A 4-hour acetaminophen level is obtained and results with a level of 180 mcg/mL. These local protocols vary from the labeled dosing; contacting and using your local poison center’s protocol is recommended.
Author: Natalie Bertrand, MD Editor: Naillid Felipe, MD Background: Definition: adverse reaction to blood product administration Incidence: more common in children than adults, except for delayed hemolytic transfusion reactions Allergic (non-anaphylaxis) – Platelets 1-3%; RBCs 0.1-0.3% mg IF requiring IM Epi >3x, switch to IV Epi, 0.05-0.1
The neighbor recorded a systolic blood pressure again above 200 mm Hg and advised her to come to the ED to address her symptoms. Both the outdated 2014 AHA/ACC guidelines and the updated 2023 ESC guidelines recommend immediate invasive management of patients with uncontrolled chest pain. She contacted her neighbor, a nurse, for help.
Scan the entirety of the affected area in 2 planes. Be aware of the patient’s comfort throughout the examination. A water bath may be helpful to visualize lesions in extremities such as the hands or feet. The probe sits just below the water’s surface and does not need to contact the skin. It may also aid in identifying nearby vasculature.
Check the pulse RSI= Resuscitation Sequence Intubation Hypoxia, Hypotension, and Acidosis are the reason patients code during/post intubation These patients are super high risk for all 4 Optimize first pass success – Induction agent + paralytic Unconscious patients will still have muscle tone Induction Ketamine or Etomidate at half doses (i.e.,
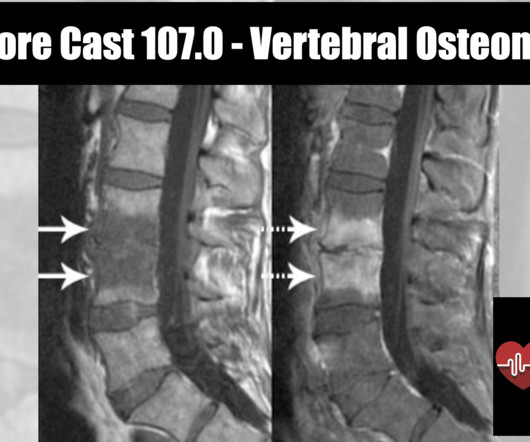
REBEL Core Cast 107.0 – Vertebral Osteomyelitis Click here for Direct Download of the Podcast Definition Inflammation of the vertebrae due to a pyogenic, fungal or mycobacterial organism. Classified as either acute (days), subacute (weeks) or chronic (months) Spondylodiscitis: a term encompassing osteomyelitis, spondylitis and discitis.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content