This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
fold higher risk of NSTI than the control group 12 For those without comorbidities , AUD exhibited a 15.2-fold fold higher risk of NSTI than the control group 12 For those without comorbidities , AUD exhibited a 15.2-fold fold higher risk of NSTI than the control group 12 For those without comorbidities , AUD exhibited a 15.2-fold
3, 4 It is the most common nosocomial infection in patients on mechanical ventilation, and one of the leading causes of nosocomial infection among all patients in the ICU. 1, 2 Its occurrence often portends worse outcomes in intubated patients, whose projected hospital course was already tenuous. 4, 8 Paper: Dahyot-Fizelier, C.,
Author: Natalie Bertrand, MD Editor: Naillid Felipe, MD Background: Definition: adverse reaction to blood product administration Incidence: more common in children than adults, except for delayed hemolytic transfusion reactions Allergic (non-anaphylaxis) – Platelets 1-3%; RBCs 0.1-0.3% mg IF requiring IM Epi >3x, switch to IV Epi, 0.05-0.1
A) Amniotic fluid embolism B) Eclampsia C) Placental abruption D) Pulmonary embolism Answer: A Amniotic fluid embolism (AFE) is a rare but potentially fatal complication of pregnancy. AFE should be considered in a patient who experiences cardiorespiratory collapse during labor or shortly thereafter.
This finding persists when looking at a number of other infections including skin and soft tissue infections (SSTI) ( First10EM ), pyelonephritis ( Strohmeier 2014 ) and even bone and joint infections ( Li 2019 ). This feels intuitive as the IV route seems like it would be stronger, faster, and fix the patient better than the oral route.
He is now stabilized, fosphenytoin is being infused, you are getting ready to ship him to the neuro-ICU and wonder if cooling him down would help. His oxygen saturation begins to drop and you decide to intubate and mechanically ventilate. Background: We have covered hypothermia a number of times on the SGEM. Reference: Legriel et al.
This has included the three large RCTs published in 2014-15 comparing early goal-directed therapy (EGDT) to usual care. It is the leading cause of death in the intensive care unit (ICU) in the US and the most expensive diagnosis. mg/dl or 107 umol/L). So, you ask yourself, is this guy really septic and should we bypass those fluids?
Check the pulse RSI= Resuscitation Sequence Intubation Hypoxia, Hypotension, and Acidosis are the reason patients code during/post intubation These patients are super high risk for all 4 Optimize first pass success – Induction agent + paralytic Unconscious patients will still have muscle tone Induction Ketamine or Etomidate at half doses (i.e.,
2018) “Sacred Pause Imitative in the ICU: A survey of ICU physicians and nurses”. 2014) “Death of a child in the emergency department” American Academy of Pediatrics. Oppressive quietness heavy with professionals’ suppressed emotions mixed with raw parental grief. That piercing parental cry rips through the room. Kapoor et al.
Since we all inhabit the same beautiful world , and sometimes we humans overtake previous habitats of animals, we inevitably will cross paths with an animal that bites us. Usually, animals bite from fear or defense of their offspring ( ex, Brown Recluse ). Sometimes it’s a beloved pet who gets surprised or has an “off” day ( Dog Bites and PTSD ).
Author: Natalie Bertrand, MD Editor: Naillid Felipe, MD Background: Definition: adverse reaction to blood product administration Incidence: more common in children than adults, except for delayed hemolytic transfusion reactions Allergic (non-anaphylaxis) – Platelets 1-3%; RBCs 0.1-0.3% mg IF requiring IM Epi >3x, switch to IV Epi, 0.05-0.1
Pertinent physical examination findings: CV: Tachycardic, regular rhythm. Lungs: Tachypneic, decreased breath sounds left lung base. Abdomen: Soft, non-tender, without rebound or guarding. What is the likely diagnosis, and what are your initial steps in evaluation and management? upper endoscopy, transesophageal echo, etc.).
They found NO difference in drain failure rates ( 11% pigtail vs 13% chest tube P=0.74), total daily volume drained or length of ICU stay between groups. You ask your anaesthetist to get ready to sedate or intubate depending on their status – Significant risk to the department – you make sure security is aware And your patient arrives.
This has been moderately well studied with MIST-2 2011 and the Picollo trial (2014) being commonly quoted trials suggesting benefit. The major barrier to implementation in the ICU setting is the almost complete absence of ICU patients from these trial cohorts. 11, 1419–1425 (2014). LDH>1000 Sugar <2.2
More common in the setting of atherosclerotic lesions than emboli, which typically occur with sudden onset of symptoms. Symptoms may range from days to months prior to stroke onset. As many as two-thirds of patients with BAO experience prodromal symptoms, including TIAs, minor strokes, or other symptoms.
The team sits down for a hot debrief once the patient is stabilised and transferred to the ICU. 2014 Jun 26;23(12):653-9. While you are leading the resuscitation, one of your senior colleagues belittles a junior staff member for struggling to site an IV line. How do you manage this situation? cognitive rehearsal techniques ).
Chronic alcohol use causes changes to preserve homeostasis, and when the stimulus is removed, alcohol withdrawal results due to decreased inhibition via the GABA system and increased excitation via the glutamate system. Tolerance to alcohol can also result in cross-tolerance to benzodiazepines and to a lesser degree barbiturates.
Time was of the essence, the patient was intubated, ACLS measures were continued, and POCUS was performed. The POCUS findings enabled EPs to confidently recognize findings consistent with hemodynamically unstable (formerly sub-massive or massive) PE. Multiorgan POCUS The diagnostic power of POCUS often resides in combining multiple ultrasound exams.
Notable Physical Exam: General: Tripoding, severe respiratory distress. However, emergency physicians have recently faced a multitude of patients requiring ETI with anatomically and physiologically difficult airways; these patients increase the risk of a can’t intubate/can’t oxygenate scenario or significant hypoxemia, hypercarbia, or acidemia.
The 48-hour group had a significantly longer length of stay in the ICU and time on mechanical ventilation amongst survivors, both of which were expected since they were kept at target temperature for longer, requiring more resources. The trial was conducted in 25 ICUs in France between 2014 and 2018. C to a goal of 36.5
Take Home Points SBO should be considered in all patients presenting with abdominal pain particularly if they have a prior abdominal surgical history Patients with SBO often have non-specific signs and symptoms. There is no history or physical exam feature that rules out the disease Lactate elevation is a late finding in SBO.
There was no difference in the secondary outcomes of time to hemostasis, ventilator-free days, ICU-free days, disposition at 30 days, incidence of primary surgical procedures, and functional status at hospital discharge (measured as Glasgow Outcome Scale-Extended Score). Clinicians were blinded to treatment until delivery of blood products.
This explorative review described insertion success rates, time to first insertion, and duration of IO function (time from insertion to IO failure, IV access insertion, transfer to ICU, or death). This time the PEM MSc team from QML , in association with DFTB, are taking over… Article 1: Insulin infusion in paediatric DKA – high or low?
Below follows a drug manual for use in the CCU (coronary care unit), ICU (intensive care unit) or ER (emergency room). J Cardiovasc Pharmacol Therap (2014). Several endogenous and synthetic agents exist and are frequently combined to achieve the desired hemodynamic outcome. Minimal chronotropic effect. Increases coronary blood flow.
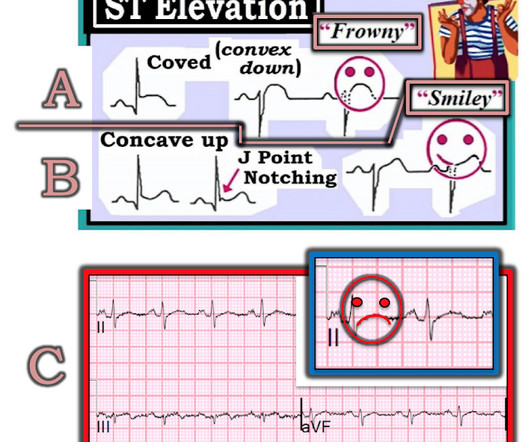
If for some reason the angiogram is delayed, they should receive maximal medical therapy in an ICU setting with continuous 12-lead ST segment monitoring under the close attention of a practitioner with advanced ECG interpretation training. The patient did well. Patel et al., Krucoff et al.) Patel et al. American Journal of Cardiology 1990.
The patient was managed in the ICU and had serial troponins. Here is data from a study we published in 2014 for type II NonSTEMI: Sandoval Y. You do NOT see this in normal variant STE, nor in pericarditis. He had no more ECGs recorded. First was 2.9 ng/mL and subsequentle dropped to 1.5 Beware of diagnosing type 2 MI.
In this situation, an ABG should be obtained periodically for correlation, though this is more relevant for the intensive care unit (ICU) setting than in routine ED care (5, 9). How would an ABG even change the initial stabilization of any of these patients? What alternative testing can be done in these circumstances?
The 2021 SSC no longer recommends the use of the quick sequential organ failure assessment (qSOFA) as a single screening tool for sepsis or septic shock compared to systemic inflammatory response syndrome (SIRS), national early warning score (NEWS), or modified early warning score (MEWS). vs. 0.91), positive predictive value (0.27
You review his chart and note that he had a heart transplant in 2014 but has not followed up with a cardiologist for at least 3 years. His vital signs on arrival include HR: 67 bpm, BP: 101/74 mm Hg, RR: 18 bpm, T: 98.3 He also developed a cough and diffuse abdominal pain over the past few days. BNP should normalize after about 2 months.
All treatments were given for the assigned time frame or until ICU discharge, whichever came first. In the control group, patients treated for severe sepsis or septic shock in the year prior to the initiation of triple therapy, hydrocortisone was used at the discretion of the intensive care unit (ICU) attending.
Left lower lung field end demonstrates expiratory wheezing on auscultation. Other lung fields unremarkable. smoke, high ozone levels, smog) Asthma/reactive airway disease (RAD) Diagnostic criteria 7,8 Respiratory symptoms +/- fever (at least 38.0 C or 100.4 mg/kg, max 4 mg per dose q20-30min) or hydromorphone (0.01-0.02 mg/kg, max 0.4 C or 100.4
What They Did: Investigators performed a retrospective cohort study in the Emergency Department at the University of Michigan between July 1, 2014 through December 31, 2018. 2 Vancomycin, in combination with either piperacillin-tazobactam or cefepime, is commonly used for empiric treatment in these cases. In 2021, Buckley et.
Disposition is often admission to an intensive care unit (ICU) setting. Questions: What is the most likely causative xenobiotic that led to these findings? Influenza vaccine Methanol Organophosphate Paraquat Are her symptoms reversible? Yes No What therapy or therapies are critical for this patient? 7 May lead to respiratory failure.
This process of sickling and unsickling goes on and off until the erythrocyte membrane is no longer flexible. Irreversible sickle cells undergo either intravascular haemolysis or extravascular removal by the reticulo-endothelial system resulting in anaemia and splenic sequestration. Blood culture is pending. How would you evaluate this child’s pain?
and the patient was given more insulin/dextrose/calcium and admitted to ICU. The reason this is clinically important is that if hypocalcemia is present, this may further exacerbate the adverse cardiac effects of hyperkalemia ( Barboza de Oliveira et al Rev Bras Cir Cardiovasc 29(3):432-436, 2014 ).
2014 Oct;31(e1):e19-24. but PPV ranges from 25.1-39.5% years Internal validation cohort: 43,400 patients with mean age 3.7 years External validation cohort: 45,855 patients with mean age 2.6 0.38 (95% CI 0.20-0.39) 0.39) AUROC of 0.71-0.92 0.92 (95% CI 0.70-0.92) and PPV of 5.3-7.1% and PPV of 22.2% but PPV ranges from 25.1-39.5% Emerg Med J.
In 2014, the Royal College of Radiologists (RCR) Paediatric Trauma Protocols were published, recommending that CT chest imaging be appropriately limited to children in specific high-risk groups. Our team have scoured the literature, so you don’t have to… or it might spark an interest to go and have a look at the full article.
Since the 2010s multiple trials have explored the feasibility of fluid restrictive resuscitation both on initial resuscitation in the ED, as well as in the intensive care unit (ICU). Tullo et al. link] During the 2017 IV fluid shortage, Patino et al. The first study was by Edna et al. The second study by Springhart et al. Tarplin et al.
Success at intubation likely takes more time and practice than other procedures, as shown in recent research on ED residents and their success rate at intubating, measured as a function of their total number of intubations (See Figure 1). Practice may not achieve perfection, but it will make you better. fiber optic through the nose).
History of Present Illness The collateral history indicates that her symptoms began one week into her journey, but medical care was inaccessible at the time. The family reports no history of food allergies, insect bites, or contact with sick individuals. The patient did not receive pre-travel prophylaxis for malaria, hepatitis A, or yellow fever.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content