
OMI in a pediatric patient? Teenagers do get acute coronary occlusion, so don't automatically dismiss the idea.
Dr. Smith's ECG Blog
DECEMBER 5, 2023
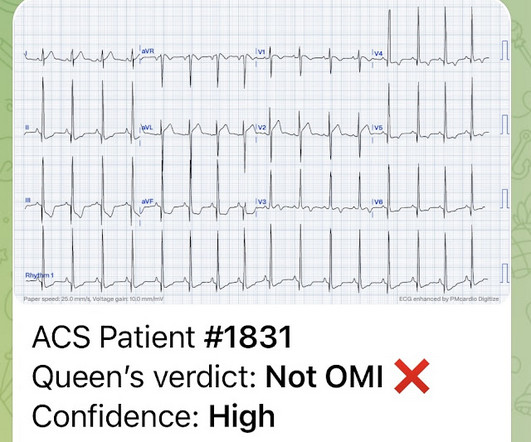
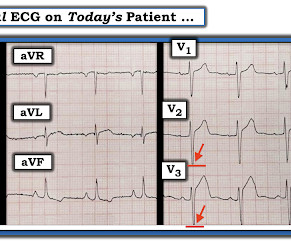
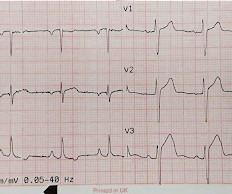
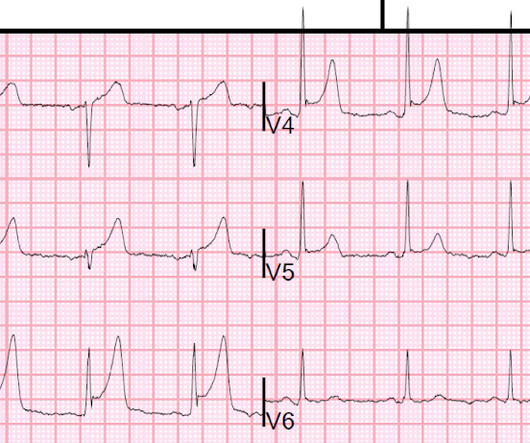
Acute coronary syndrome in a pediatric patient? An ECG was perfomed on arrival to our ED: NSR with ST elevation II,III, aVF with reciprocal depression in aVL Would you refer this pediatric patient for emergent PCI? 2016 Apr 12;67(14):1738-49. Ultimately, cardiac cath was done — revealing patent coronary arteries.



















Let's personalize your content