

Acute OMI or "Benign" Early Repolarization?
Dr. Smith's ECG Blog
DECEMBER 27, 2023
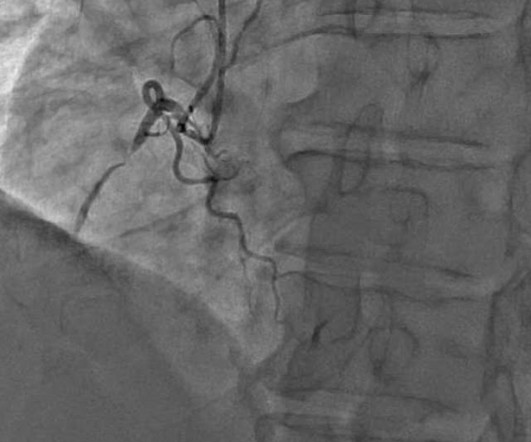
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergency department at around 3 AM complaining of chest pain onset around 9 PM the evening prior. ECG 1 What do you think? Grines, C.



















Let's personalize your content