

Sudden shock with a Nasty looking ECG. What is it?
Dr. Smith's ECG Blog
MAY 3, 2024
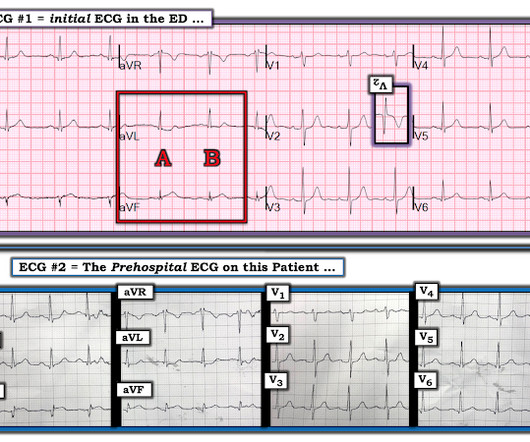
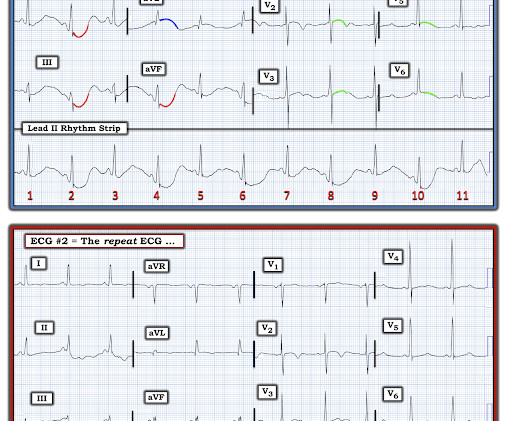
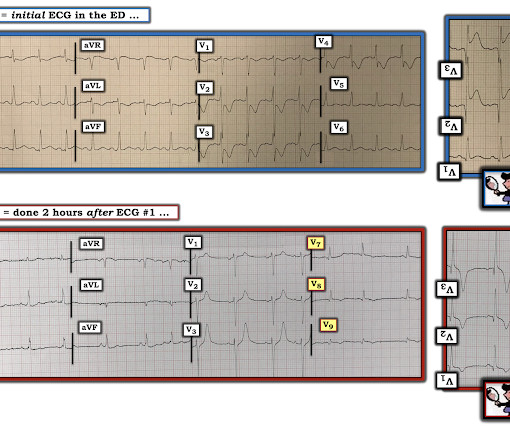
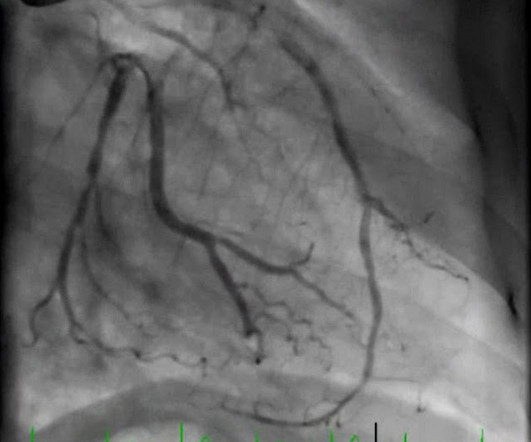
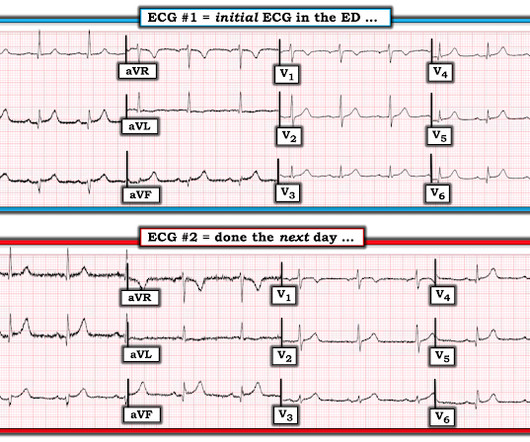
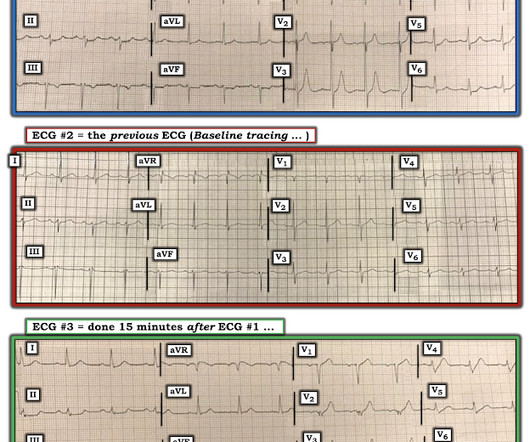
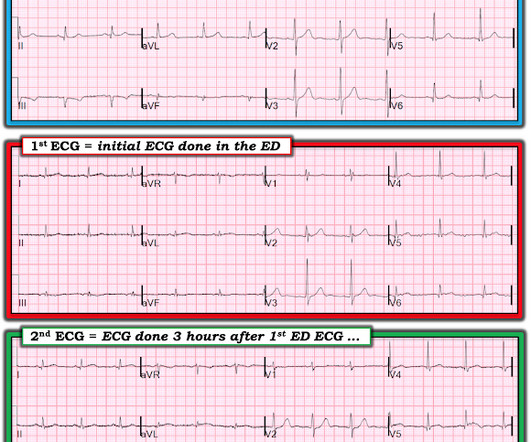
But this time the Queen gets it wrong (thinks it is not OMI): There were runs of VT: Tha patient arrived in profound shock and had an ED ECG: Now there is some evolution to include the ST elevation (rather than ST depression) in V4-V6. RBBB + LAFB in the setting of ACS is very bad. Posterior and high lateral OMI. Learning Points: 1.




































Let's personalize your content