This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
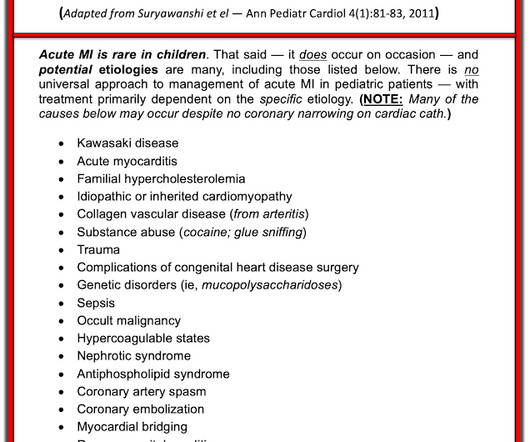
Acute coronary syndrome in a pediatric patient? Ultimately, cardiac cath was done — revealing patent coronary arteries. Figure-1: Potential Causes of acute MI in Children ( Adapted from Suryawanshi et al — Ann Pediatr Cardiol 4(1):81-83, 2011 ). Smith : this was the prudent thing to do!!
Date: September 8th, 2021 Reference: Desch et al. Date: September 8th, 2021 Reference: Desch et al. Defibrillation is the treatment of choice in these cases but does not often result in sustained ROSC ( Kudenchuk et al 2006). Acute coronary syndrome (ACS) is responsible for the majority (60%) of all OHCAs in patients.
Additional architectural changes include systolic anterior motion of the mitral valve, endothelial dysfunction at the level of the coronary arterial bed, and ventricular diastolic dysfunction. This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. It is spread to V2 and V3. References Naidu, S.
The coronary angiogram revealed no critical stenosis, or acute plaque ulceration. Takotsubo should be a diagnosis of exclusion after angiography reveals no obstructive coronary disease, and repeat Echo displays left ventricular recovery. Furthermore, pertinent electrolyte values (e.g. potassium) were within normal parameter.
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction. This is not the case.
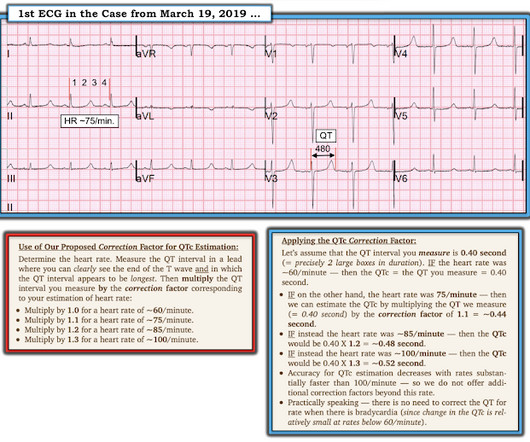
Bogossian et al. (1) Bogossian H, Frommeyer G, Ninios I, Hasan F, Nguyen QS, Karosiene Z, Mijic D, Kloppe A, Suleiman H, Bandorski D, et al. Among patients with left bundle branch block, T-wave peak to T-wave end time is prolonged in the presence of acute coronary occlusion. Then we can correct that modified QT for heart rate.
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). link] [1] Zachary et al. Utility of the history and physical examination in the detection of Acute Coronary Syndromes in emergency department patients. Western Journal of Emergency Medicine, 18 (4), 752-760. [2]
Cardiology admitted him for observation with plans for next-day coronary angiogram. Unfortunately, due to the patient’s abrupt exodus from the PCI center – without benefit of coronary angiogram, or echo, for example – the disposition will forever remain unknown. [1] 1] Driver, B. Emergency Medicine Journal, 1-5. [2] 3] Niu, T.,
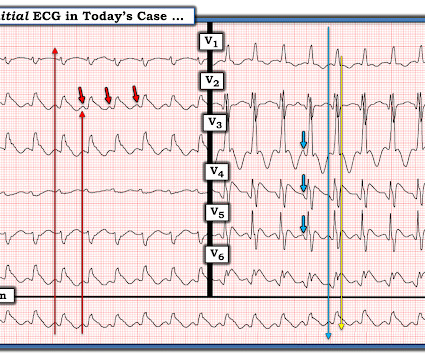
Below is the version standardized by PM Cardio app Meyers interpretation: Findings are specific for posterior (and also likely inferior) wall transmural acute infarction, most likely due to acute coronary occlusion (OMI). Most OMI have a peak Troponin T over 1000 ng/L [reference: Baro R et al. Clinical Cardiology 2019.
It shows a proximal LAD occlusion, in conjunction with a subtotally occluded LMCA ( Left Main Coronary Artery ). Upon contrast injection of the LMCA, the patient deteriorated, as the LMCA was severely diseased and flow to all coronary arteries ( LAD, LCx and RCA ) was compromised. He was taken immediately to the cath lab.
Coronaries were clean. Not OMI with High Confidence Click here to sign up for Queen of Hearts Access We showed that the Queen of Hearts decreases false positive cath lab activations: 1) Published recently in Prehospital Emergency Care Baker PO et al. 2) To be presented at AHA conference in Chicago in 2 weeks: Sharkey SW et al.
The proof of this is that only 5% of patients enrolled had acute coronary occlusion. Lemkes JS, Janssens GN, van der Hoeven NW, et al. Coronary Angiography after Cardiac Arrest without ST-Segment Elevation. We at Hennepin recently published this study Sharma et al. This study failed to do so. 5% vs. 58%!! 5% vs. 58%!!
He underwent coronary angiography which showed severe multivessel disease, and he agreed to proceed with workup for CABG. The September 27, 2019 post — for the Rowlands & Moore article with the above-noted formulas for recognizing the “culprit” extremity. The September 22, 2019 post — intermittent ST-T wave artifact.
Cardiology was consulted, who advised to surveil a metabolic process as this did not strike them as acute coronary syndrome. No calcium was administered during pre-hospital transport. The following ECG was captured upon arrival at the receiving ED. The serum K returned 8.7, along with a pH 6.94, and an HCO3 of 5. 2] Birnbaum, Y., Physiology.
First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion. The new ACC expert consensus explains that: “STEMI ECG criteria on a standard 12-lead ECG alone will miss a significant minority of patients who have acute coronary occlusion. Take home 1.
The TOMAHAWK (Desch 2021), COACT (Abella 2019), and PEARL (Lemkes 2019) trials examined patients with OHCA without ST elevation with a shockable rhythm, and investigators found no difference in delayed versus emergency angiogram. Article: How-Berlemont C, Lamhaut L, Diehl J, et al. Additionally, the trial had several biases.
The biphasic T wave is consistent with recent reperfusion of an occluded coronary artery supplying the inferior region. Here’s the angiogram of the RCA : No thrombus or plaque rupture in the RCA (or any coronary artery) was found. This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA.
Dr. Smith’s ECG Blog has published a growing list of over 40 cases of ECGs falsely labeled ‘normal’ by the computer which are diagnostic of Occlusion MI, and Smith et al. Smith’s ECG Blog has published a growing list of over 40 cases of ECGs falsely labeled ‘normal’ by the computer which are diagnostic of Occlusion MI, and Smith et al.
Hgb 11g/dL (110g/L) and leukocytosis, and a mildly elevated troponin (36 ng/L, with normal 1mm STE in aVR due to ACS will require coronary artery bypass surgery for revascularization, the infarct artery is often not the LM, but rather the LAD or severe 3-vessel disease. Harhash AA, Huang JJ, Reddy S, et al. Knotts et al.
His medical history includes hypertension, a decade-long battle with diabetes, ischemic heart disease, a coronary bypass graft surgery ten years ago, a diagnosis of congestive heart failure for the last five years, and a prior ICD implantation five years ago.
Their OMI Manifesto details how use of standard STEMI criteria results in an unacceptable level of inaccuracy, in which an estimated 25-30% of acute coronary occlusions are missed! The article by Aslanger, Smith et al that is featured above in today’s post has just been published. P.S.: Our September 3, 2020 post features Dr.
Smith presented results from a 2019 article by Harhash et al, that confirm how the ECG pattern shown in Figure-1 does not represent acute LMain occlusion — but rather the differential diagnosis that I show above. Today’s Post by Dr. Smith adds to our knowledge of this syndrome.
But the stuttering pain and sudden onset suggest acute coronary occlusion (Occlusion MI, or OMI). Cath lab activation by the ED and I agree with coronary angiography emergently." Result: no angiographically significant obstructive coronary artery disease. Smith and Meyers to diagnose both obvious (STEMI) and subtle OMI.
Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al. It can only be seen by IVUS. MINOCA has many etiologies.
By Magnus Nossen, edits by Grauer and Smith The patient is a 70-something female with DMII, HTN and an extensive prior history of coronary artery disease and myocardial infarctions. PLUS — Today's patient is an older woman with known severe coronary disease who presented with new chest pain. She's had multiple PCI procedures.
I have here 38 cases of "Computer Normal" ECGs which were critically abnormal and the vast majority are missed acute coronary occlusions (Missed Acute OMI) and most were recognized by the physician. We wrote this Editorial in the Journal of Electrocardiology in 2019. Litell JM, Meyers HP, Smith SW.
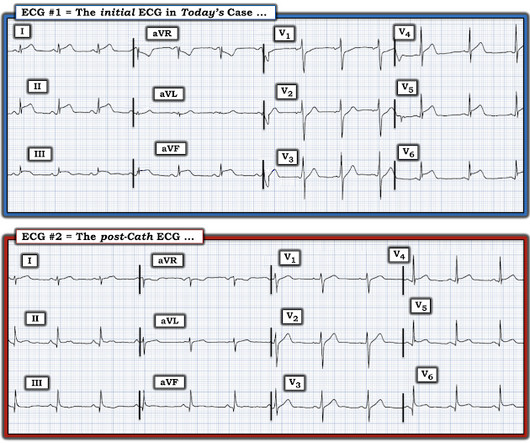
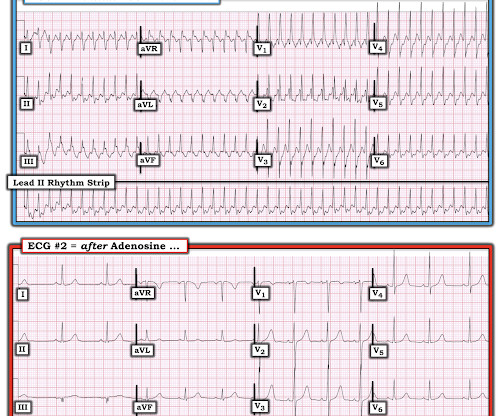
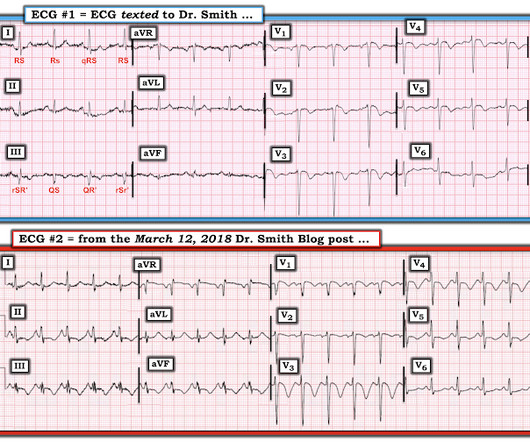
Coronaries were normal, as was serial troponin. I sent the initial ECG of both cases without any context to my colleague Mazen El-Baba, a senior EM resident with an interest in ECG interpretation, and he responded: “RBBB with first degree AV block” for the first (ie no acute coronary occlusion), and “RBBB and superimposed OMI” for the second.
It was a 60yo with a history of stents to the circumflex and right coronary arteries, who presented with 9 hours of fluctuating central chest pain. This is step 4 : relying on the first troponin level to rule out acute coronary occlusion. 4] CT revealed no dissection but extensive coronary atherosclerosis. J of Emerg Med 2021.
And so it is wise to look at the coronary arteries. This ECG certainly looks like myocarditis, and was due to myocarditis, but missing acute coronary occlusion is not acceptable. 3–8 Shi et al. In acute MI, the T-wave is large, and the T/ST ratio is high. This is much more typical of myocarditis. Angiogram was negative.
Because of the importance of this entity — we continue to periodically review it in cases we present ( See the May 2, 2019 post — among many others ). NOTE: For illustrative purposes — I’ve adapted Figure-1 from the original manuscript by de Winter et al, published in this 2008 NEJM citation. D e W inter T Waves : In 2008 — Robert J.
16 In a study conducted by Millet et al. A retrospective study done in May 2023, by Shaish et al 24 showed a 30 % reduction in accuracy of NCCT compared to CECT in a study done among 201 adult ED patients with abdominal pain. link] Bellolio MF, Heien HC, Sangaralingham LR, et al. link] Published May 26, 2022. West J Emerg Med.
This vasoconstriction affects pretty much all the vasculature including things like the coronaries (not so good) but does seem to spare the pulmonary arteries meaning it may be good in those with pulmonary hypertension. First up is the VASST trial, (Russel et al 2008 NEJM). Nagendran 2019 in CCM. Gordon, A. Nagendran, M.
Meyers et al. Accuracy of OMI findings versus STEMI criteria for diagnosis of acute coronary occlusion myocardial infarction. Aslanger et al. DIagnostic accuracy oF electrocardiogram for acute coronary OCClusion resulTing in myocardial infarction (DIFOCCULT study). Lemkes et al. Bergmark et al.
I believe this is by far the most common outcome for this patient around the world in 2019. Current practice ranges widely, but based on my short experience and reports from other institutions, most of these patients are not being taken emergently to the cath lab in 2019. Patel et al., Krucoff et al.) Patel et al.
Karwowski et al showed that only 64% of 4581 STEMIs had TIMI 0 flow on angiogram. [25] 25] Stone et al found that 72% have TIMI 0 or 1 flow. [26] 26] Finally, Cox et al found that 80% had TIMI 0, 1, or 2.27 Karwowski et al showed that only 64% of 4581 STEMIs had TIMI 0 flow on angiogram. [25] Pol Arch Intern Med.
Backus BE, Six AJ, Kelder JC, et al. Moumneh T, Sun BC, Baecker A, et al. Identifying patients with low risk for acute coronary syndrome without troponin testing: validation of the HEAR score. Shah ASV, Anand A, Sandoval Y, et al. Patel J, Alattar F, Koneru J, et al. Gulati M, Levy P, Mukherjee D, et al.
Therefore the impulse must have originated somewhere lower in the atria, perhaps near the coronary sinus. The September 27, 2019 post — for the Rowlands & Moore article with the above-noted formulas for recognizing the “culprit” extremity. Complete heart block is the state of the AV node. The January 30, 2018 post — for PTA.
Ct coronary angiogram showed normal coronary arteries. Smith note: I think CT coronary angiogram is reasonable with the elevated troponins and symptoms. The Cardiorespiratory Implications of Ultra-marathon Bjørkavoll‐Bergseth et al. Paana et al. International Journal of Cardiology 2019. ng/L; 3 hours, 38.3
Article: Kumar M et al. Hayes-Larson 2019). References De Pietri L, Bianchini M, Montalti R, et al. PMID: 31229583 Kumar M, Ahmad J, Maiwall R, et al. PMID: 31148204 Rout G, Shalimar, Gunjan D, et al. PMID: 20335313 Wang SC, Shieh JF, Chang KY, et al. Hepatology. 2020;71(1):235-246. Hepatology. Hepatology.
SVT misdiagnosed as panic disorder Lessmeier TJ, Gamperling D, Johnson-Liddon V, et al. Lessmeier et al. I’ll add here 2 more reference links on the subject — by Brugada; Diez — and — by Tondo et al. Not all forms of idiopathic VT are predictable based on their ECG appearance ( Anderson et al, 2019 ).
Kosuge et al. Witting et al. This does not contradict the conclusions of Kosuge et al. , Finally, Stein et al. This is a paper worth reading : Marchik et al. These points have been emphasized in many previous posts on Dr. Smith’s blog ( See the April 5, 2019 post , including My Comment at the bottom of that page ).
Some excellent references on ARVD: This is a case report with lots of good info, from 2019, but you can only read it if you have a subscription to American J Cardiol: Holshouser JW and Littmann L. Here is an explanation of the importance of leads V1 and V2. Here is another nice example. Cardiac MRI will tell you if ARVC is or is not present.
This is most consistent with ischemia/infarction in the distribution of the left circumflex coronary artery. Meyers, Bracey, Smith, et al. Echocardiogram: The estimated left ventricular ejection fraction is 34% Regional wall motion abnormality-lateral, akinetic. Next Day ECG: T waves in V2, V3 are larger than they were at baseline.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content