
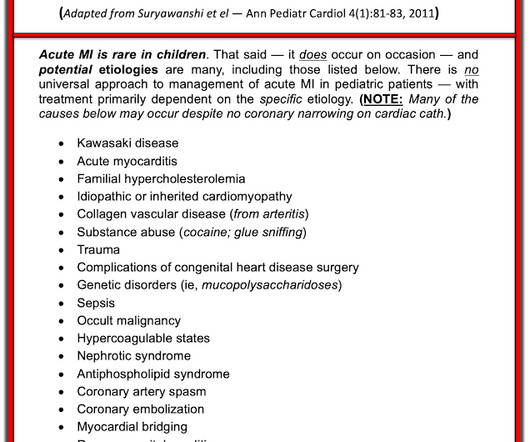
OMI in a pediatric patient? Teenagers do get acute coronary occlusion, so don't automatically dismiss the idea.
Dr. Smith's ECG Blog
DECEMBER 5, 2023
Acute coronary syndrome in a pediatric patient? He did have a family history notable for early CAD. hematological disorder like sickle cell or antiphospholipid syndome, family history of CAD or hypercholesterolemia, prior history of vasculopathies such as Kawasaki Disease, MIS-C, prior cardiac surgery, etc.)















Let's personalize your content