
OMI in a pediatric patient? Teenagers do get acute coronary occlusion, so don't automatically dismiss the idea.
Dr. Smith's ECG Blog
DECEMBER 5, 2023
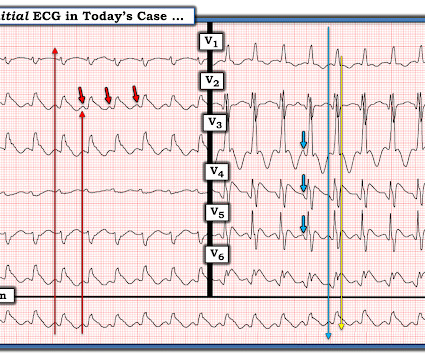
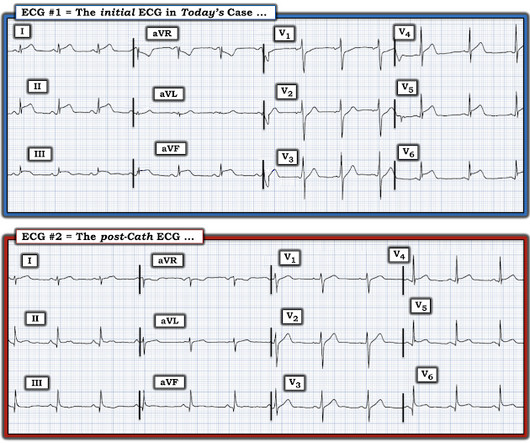
Acute coronary syndrome in a pediatric patient? Ultimately, cardiac cath was done — revealing patent coronary arteries. Written by Kirsten Morrissey, MD with edits by Bracey, Grauer, Meyers, and Smith An older teen was transferred from an outside hospital with elevated serum troponin and and ECG demonstrating ST elevations.











































Let's personalize your content