

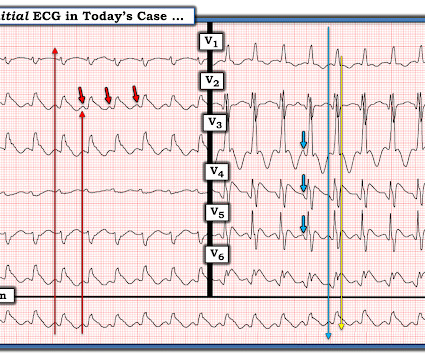
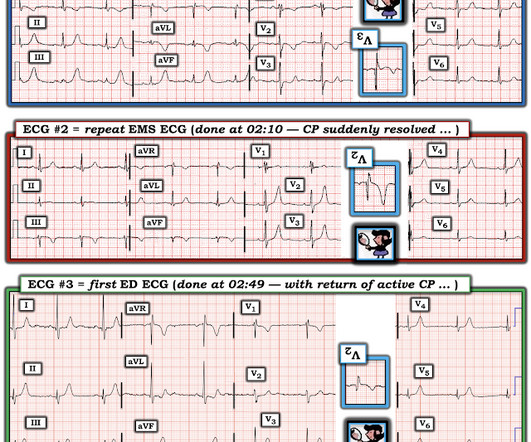
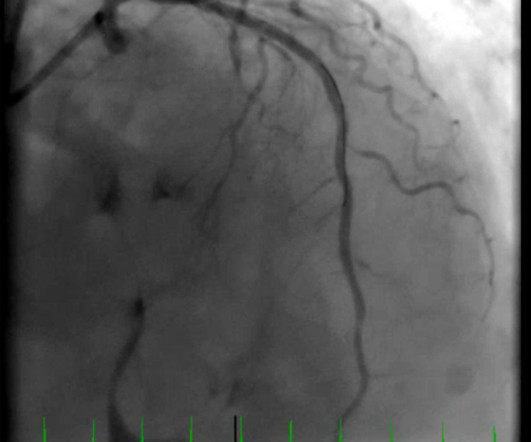
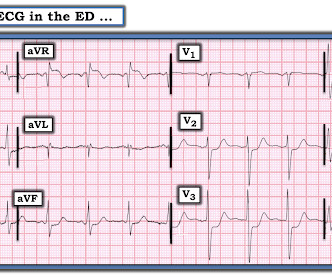
What does the angiogram show? The Echo? The CT coronary angiogram? How do you explain this?
Dr. Smith's ECG Blog
NOVEMBER 15, 2023
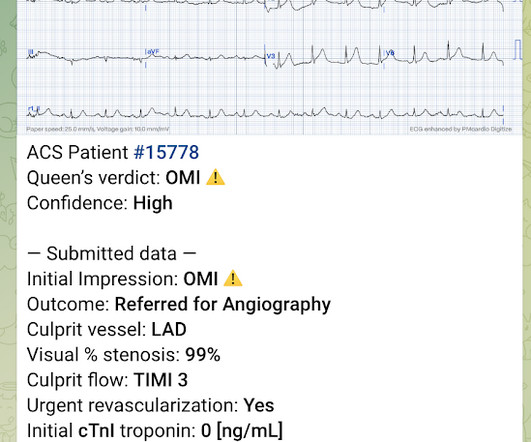
Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. CORONARY ARTERIES: Exam was not directly tailored for coronary artery evaluation, noting recent diagnostic coronary angiogram.







































Let's personalize your content