

Guidelines would (erroneously) say that this patient who was defibrillated and resuscitated does not need emergent angiography
Dr. Smith's ECG Blog
JUNE 27, 2024
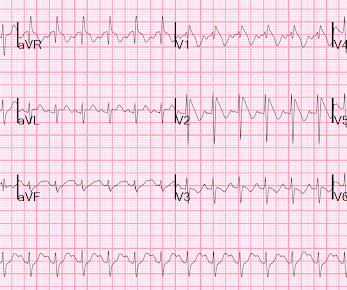
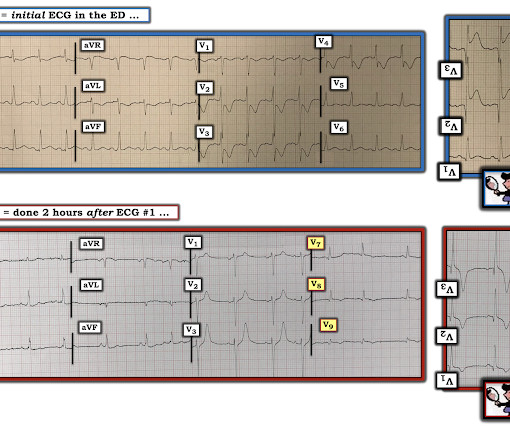
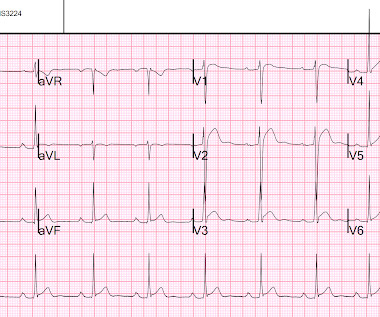
A patient had a cardiac arrest with ventricular fibrillation and was successfully defibrillated. Here was his initial ED ECG: Formal interpretation by interventional cardiologist: There is "Non-diagnostic" ST Elevation in V2-V4 and aVL. Lemkes JS, Janssens GN, van der Hoeven NW, et al.



















Let's personalize your content