

Guidelines would (erroneously) say that this patient who was defibrillated and resuscitated does not need emergent angiography
Dr. Smith's ECG Blog
JUNE 27, 2024
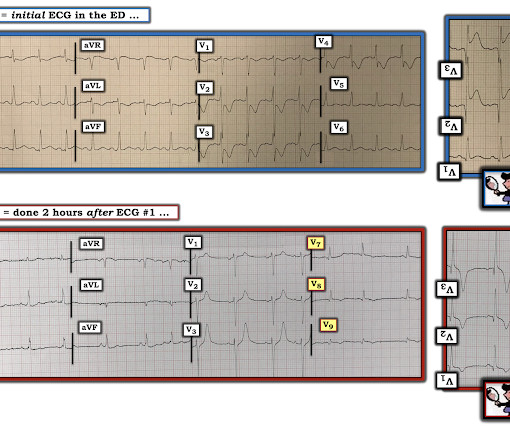
A patient had a cardiac arrest with ventricular fibrillation and was successfully defibrillated. COACT: The COACT trial was fatally flawed, and because of it, many cardiologists are convinced that if there are no STEMI criteria, the patient does not need to go to the cath lab. Lemkes JS, Janssens GN, van der Hoeven NW, et al.















Let's personalize your content