This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The 2022 American College of Cardiology (ACC) pathway provides timely guidance [1]. Encourage your ED to set up an algorithm that you can follow based on your laboratory’s assay. Low-risk patients do not routinely require stress testing in the ED. We help you translate this to your clinical practice, by illustrating with a case.
Our experience: Traditionally, ED physicians do not like ordering urine drug screens (UDS). In our study, we used COWS alone in the ED, which does utilize restlessness, anxiety, and tachycardia as part of the formula, as the sole evaluation tool for tranq dope withdrawal. Some patients require re-dosing in the ED. 2023 [book].
What Your Gut Says: The patient has a tachydysrhythmia which may be the presentation of acute coronary syndrome (ACS) even though the patient has no ischemic symptoms. Up to 80% of patients will have at least one troponin sent ( Gabrielli 2022 ). SVT is not a presenting dysrhythmia consistent w/ ACS. Cardiol Rev.
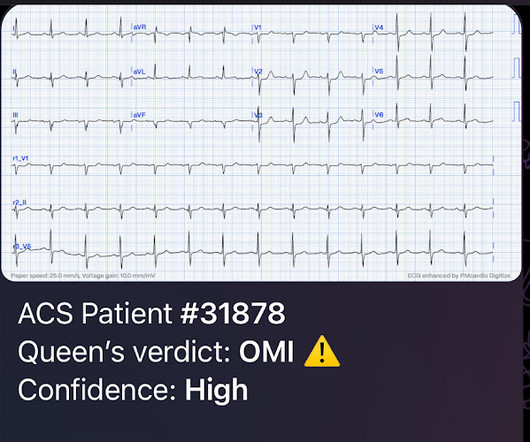
male presents to the ED at 6:45 AM with left sided chest dull pressure that woke him up from sleep at 3am. He arrived to the ED at around 6:45am, and stated the pain has persisted. Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. The pain radiated to both shoulders.
Date: June 30th, 2022 Reference: McGinnis et al. AEM June 2022. Date: June 30th, 2022 Reference: McGinnis et al. AEM June 2022. Case: You are working a shift in your local community emergency department (ED) when a 47-year-old male presents with chest pain. If we thought about ACS, we brought them in.
Other causes of sickling: acidosis, dehydration, inflammation, infection, fever, and blood stasis Sickling leads to vascular occlusion, end-organ ischemia, and decreased RBC lifespan, which, in turn, leads to pain crisis, acute anemia, sequestration, infection, and acute chest syndrome (ACS.) Each episode of ACS has a 9% mortality rate.
However, many institutions’ surgical teams still require or request a formal study over a bedside exam, likely due to a lack of confidence in the accuracy of POCUS, resulting in longer ED stays. Published 2022 Sep 2. ACS surgeons appeared to select surgery as their initial choice substantially more frequently than other subspecialties.
Sickling leads to vascular occlusion, end-organ ischemia, and decreased RBC lifespan, which, in turn, leads to pain crisis, acute anemia, sequestration, infection, and acute chest syndrome (ACS). ACS is lung injury due to vaso-occlusion in the pulmonary vasculature; many with ACS will have a concomitant vaso-occlusive pain crisis.
Date: May 24th, 2022 Reference: Broder et al. Date: May 24th, 2022 Reference: Broder et al. AEM May 2022 Guest Skeptic: Dr. Justin Morgenstern is an emergency physician and the creator of the #FOAMed project called First10EM.com Case: A 33-year-old male presents to the emergency department (ED) complaining of abdominal pain.
The person I was texting knows implicitly based on our experience together that I mean "Definite posterior OMI, assuming the patient's clinical presentation is consistent with ACS." The interventional cardiologist then canceled the activation and returned the patient to the ED without doing an angiogram ("Not a STEMI").
Cardiology consult note written around that time documents that "Pain improved with NTG, morphine in ED but still present." As a result, even before looking at this patient's initial ECG — he falls into a high -prevalence likelihood group for ACS ( for an A cute C oronary S yndrome ). Repeat cTnI drawn at around 8 AM was 3.910 ng/mL.
Written by Jesse McLaren A 75 year-old patient with diabetes and end stage renal disease was sent to the ED after dialysis for three days of nausea, vomiting, loose stool, lightheadedness and fatigue. But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. Below is the 15 lead ECG.
The neighbor recorded a systolic blood pressure again above 200 mm Hg and advised her to come to the ED to address her symptoms. Smith : As Willy states, ACS with persistent symptoms is a guideline recommended indication for <2 hour angio (both ACC/AHA and ESC). She contacted her neighbor, a nurse, for help. Clin Cardiol [Internet].
[link] Case continued She arrived in the ED and here is the first ED ECG. Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. I don't know if her pain was getting better or not.
Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? Cardioversion will address the rhythm problem immediately, also if the chest discomfort subsides when SR is restored, ischemia from ACS becomes much less likely. This patient presented to the ED “after a couple of days of chest discomfort”.
Key: Consider eclampsia in any pregnant and postpartum woman presenting to the ED, especially in patients with symptoms such as headache, confusion/altered mental status, vision changes, and hypertension. ED Evaluation: Assessment focuses on looking for complications and mimics. 2022 Aug;58:223-228. Wilkerson RG, Ogunbodede AC.
Prior episodes had simply resolved after brief symptoms, but the current episode had lasted for 2 hours without improvement, so she presented to the ED. At triage she stated her pain is still persistent, but it is mildly improved compared to when she decided to come to the ED. No diaphoresis or vomiting. How to Check Your Findings.
Episode 108: Unexplained Sinus Tachycardia Mental Model Background: When a patient in the ED has sinus tachycardia our job as emergency physicians is to identify and treat of the underlying pathology. Lactate Troponin Could this be ACS or myocarditis? In the ED, our job is to identify and treat underlying causes. Clin Cardiol.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. In our opinion it should not be given in ACS unless you are committed to the cath lab. Published 2022 Feb 20. 2022.01.006 6.
Here is the first ED ECG recorded, now pain free after sublingual Nitro: There is what appears to be a reperfusion T-wave in I and aVL. For examples of this phenomenon — See My Comment in the February 14, 2018 — July 21, 2020 — and December 22, 2022 posts in Dr. Smith's ECG Blog ). So they looked into the patient's chart.
Arch Dis Child Fetal Neonatal Ed. 2023 Apr 20:fetalneonatal-2022-324835. Arch Dis Child Fetal Neonatal Ed. 2023 Apr 4:archdischild-2022-325281. De Alwis AC, et al. Effect of initial and subsequent mask applications on breathing and heart rate in preterm infants at birth. Kuypers KLAM, et al. Hegeman EM, et al.
The NIHSS cutoff that predicts outcomes is 4 points higher in AC compared with PC infarctions. Median time from ED arrival to diagnosis was 8 hours 24 min in one study, with only 19% being diagnosed within the 4.5-hour Updated 2022 Dec 22]. Updated 2022 Oct 15]. Post TW, ed. hour IV thrombolytic window.
FIGURE 1: First ED EKG. FIGURE 2: Baseline ED from 2 months prior. FIGURE 3: Second ED EKG. Considering hyperacute T-waves have been accepted as STEMI equivalents, it is possible that pseudonormalization could gain more recognition as an indicator of ACS. 2022 Nov, 80 (20) 1925–1960. Click to enlarge.)
Smith: If this is ACS (a big if), t his is just the time when one should NOT use "upstream" dual anti-platelet therapy ("upstream" means in the ED before angiography). History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. Anything more on history?
Case "Male, 43yo, come to ED with Epigastric Pain started 3 hours ago. Remember: these findings above are included as STEMI equivalent findings in the 2022 ACC Expert Consensus Decision Pathway on ACS Patients in the ED. Since then, I started looking for OMI EKG findings and not just STEMI. Risk Factors: High Cholesterol.
He reportedly told his family "I think I'm having a heart attack", then they immediately drove him to the ED, and he was able to ambulate into the triage area before he collapsed and became unresponsive. CPR was initiated immediately. It was reportedly a PEA arrest; there was no recorded V Fib and no defibrillation.
All you know, back in ED, is that the ETA is 10 minutes, and there is a single stab wound to the chest. The ODP is caught up leaving theatres and has not yet made it down to ED. Back in ED with Ranulf, and pack two has gone through. 2022 Dec;57(12):986-993. Trials 23, 384 (2022). The trauma call goes out.
Background Information: Atrial fibrillation with rapid ventricular rate (RVR) is one of the many tachydysrhythmias we encounter in the Emergency Department (ED). The average time to control HR in the IV amiodarone was 1.7h, which is usually the average time for disposition from the ED. Paper: Mason JM, et al. Am J Emerg Med.
A 44 year-old male with unknown past medical history came by emergency medical services (EMS) to the emergency department (ED) for an electrical injury and fall from a high voltage electrical pole. 2,3,5 Except for laundry or electrical car outlets (240 V AC), all U.S. household outlets are rated at 120 V AC. 2023 Jul 17.
The patient vomited once and given the more intense pain decided to come to the ED. Clin Cardiol 2022; [link] Labs included: hsTnI 156 ng/L, Hb 12 g/dL, WBC 12x10^9/L, Cr. Smith comment: We have shown that use of opiates is associated with worse outcomes in ACS: Bracey, A. No history of GIB, dysuria, or GU symptoms. mg/dL, K 3.5
The ECG is diagnostic for acute transmural infarction of the anterior and lateral walls, with LAD OMI being the most likely cause (which has various potential etiologies for the actual cause of the acute coronary artery occlusion, the most common of which is of course type 1 ACS, plaque rupture with thrombotic occlusion).
ED treatment should focus on airway, breathing, and circulation with consideration for cervical spine protection depending on the circumstances surrounding the event. References Webb AC, Wheeler A, Ricci A, et al. Johnson MB, Boriack ED, McConnell CM, et al. 4 Another study cited only 2.3 South Med J. 2021;114(5):266-270.
About an hour later, he was then found on the floor in cardiac arrest in the ED. ST depression maximal in V1-V4, in the context of ACS symptoms and unexplained by QRS abnormality or tachydysrhythmia, should be considered posterior OMI until proven otherwise. His initial troponin T was 15 ng/L (only two hours since pain onset).
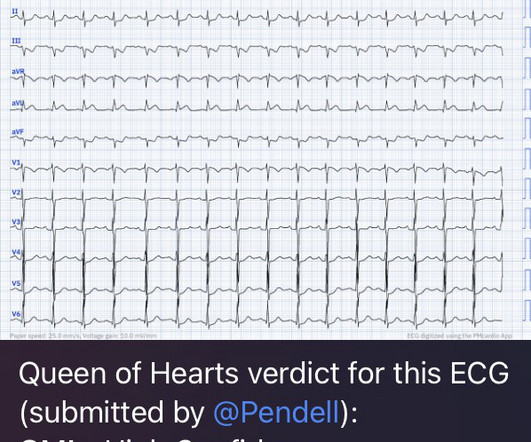
One case sent by Dr. Sean Rees MD, written by Pendell Meyers, other case by Sam Ghali and Steve Smith Take a look at these two ECGs below from two patients in the ED, first without any clinical context. He had no symptoms of ACS. Full case details and outcomes are below. Case 1: Case 2: Case 1: What do you think? Physician: "No STEMI."
It has been well over a year since the controversial publication of the Agency for Healthcare Research and Quality (AHRQ) report on diagnostic errors in the emergency department (ED). percent of ED visits resulted in preventable death as result of diagnostic error. Available from: [link] Newman-Toker DE, Nassery N, Schaffer AC, et al.
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. Most studies examine undifferentiated ACS cohorts, with only a handful providing separate data. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al.
A 60 year old with chest pain presented to the ED. In the December 5, 2022 post of Dr. Smith's ECG Blog — We show 4 additional cases of this pulse-tap artifact. Finally, as I discuss in My Comment in the August 26, 2022 post ( which applies the electrophysiologic principles of Rowlands & Moore: J. This is no longer the case!
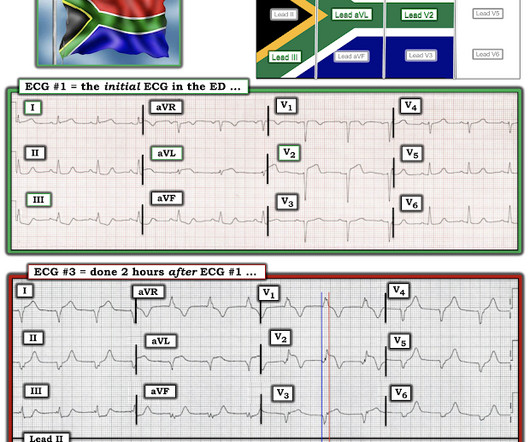
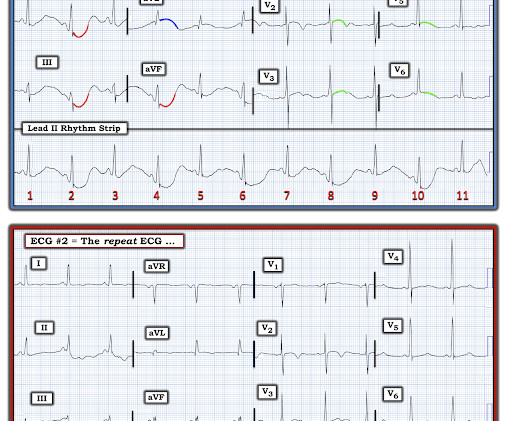
It was shown to me with worry for ischemic ST elevation, which is certainly possible from severe CO toxicity, or concomitant ACS. Figure-1: Comparison of the initial ECG in the ED ( = ECG #1 ) with the follow-up ECG done the next day ( = ECG #2 ). Routine ECG recorded before hyperbaric therapy.Are they related?
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chest pain. Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. I cannot be anything else.
Corroborating this is the subtle ST depression in V2-V3 which is inappropriate for the normal QRS complex, and in the context of ACS, we have shown this is quite specific for posterior OMI. In the context of ACS, ST depression maximal in V1-V4 (rather than V5-V6) not due to a QRS abnormality is specific for posterior OMI.
Recall that, in the setting of ACS symptoms, ST depression that are maximal in leads V1-V4 (as opposed to V5 and V6) not attributable to an abnormal QRS complex is specific for OMI. That this might happen should not be surprising — since the patient's chest pain was already ongoing for 3 hours prior to arrival in the ED.
Here is her ECG on arrival to the ED: What is your differential? Cardiothoracic and vascular surgery were consulted and the patient was taken to the OR within an hour and a half of her arrival to the ED. Her initial ED high sensitivity troponin was less than 6ng/L (below limit of detection), and none further were ordered.
After discussing all of the above with ED staff, we have made a decision to get stat echocardiogram and assess overall LV function and wall motion abnormalities and defer cath lab activation at the time." Precordial Swirl in ECG #1: As discussed in the October 15, 2022 post in Dr. Smith's ECG Blog — Drs. It does not radiate.
CT Coronary angiogram is usually used to make ACS much less likely in the context of a patient who is ruled out for acute MI by troponins. Thus, Wellens' syndrome should be thought of as a transient OMI or transient STEMI. Transient STEMI is at high risk of re-occlusion.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content