This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
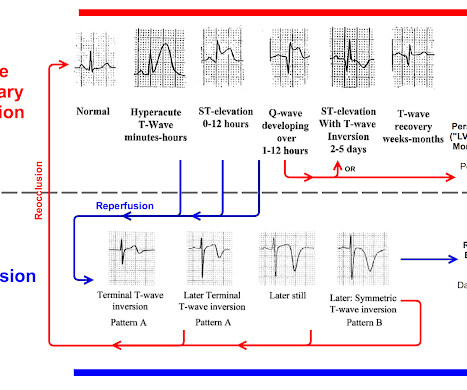
The 2022 American College of Cardiology (ACC) pathway provides timely guidance [1]. Applying the 2022 ACC guideline Before delving into the specifics of the hs-cTn pathways, start with the ECG. The ACC 2022 pathway has a section dedicated to ECGs in ischemia [1], and FOAMcast has a great visual summary.
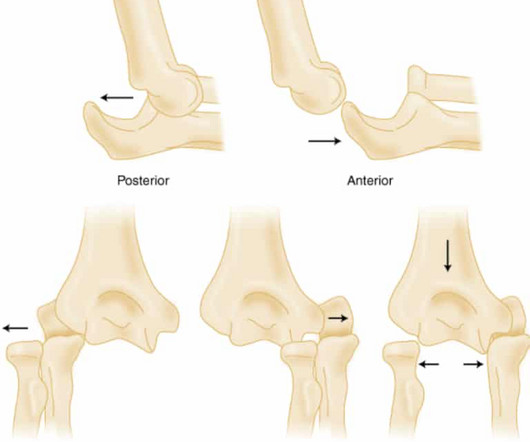
Elbow Dislocation Definition: Disarticulation of the proximal radius & ulna bones from the humerus Epidemiology: Incidence Second most common joint dislocation (after shoulder) in adults Most commonly dislocated joint in children Accounts for 10-25% of all injuries to the elbow ( Cohen 1998 ) Posterolateral is the most common type of dislocation (..)
The biggest change has been the gradual replacement of diacetylmorphine (heroin) by fentanyl and other synthetic opioids. Along the same time, a veterinary sedative, xylazine , became popular in Puerto Rico in individuals who used injection drugs [3]. We treat with wound care and reserve surgical management only for limbs that are no longer viable.
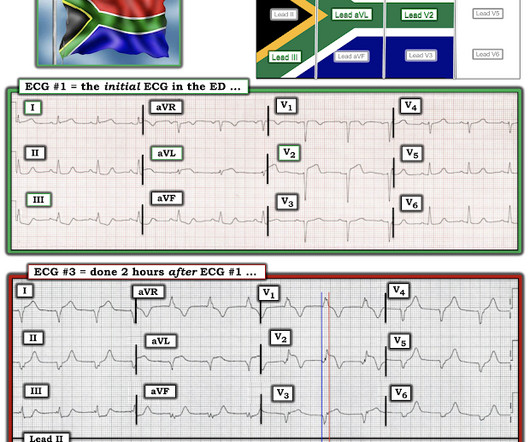
Review of the 2 ECGs in today's case is insightful ( Figure-1 ): The initial ECG shows sinus rhythm, LAHB and meets Peguero Criteria for LVH ( See My Comment in the August 15, 2022 post of Dr. Smith's ECG Blog for more on LVH criteria ). Thus, the lumen observed may actually still be the same size as the original, normal lumen.
As a result, even before looking at this patient's initial ECG — he falls into a high -prevalence likelihood group for ACS ( for an A cute C oronary S yndrome ). We therefore need to assume and rule "out" ACS — more than having to rule it "in". V2 has some changes, but at least to me it is not as clear what to make of them. Shmueli, H.,
What Your Gut Says: The patient has a tachydysrhythmia which may be the presentation of acute coronary syndrome (ACS) even though the patient has no ischemic symptoms. Up to 80% of patients will have at least one troponin sent ( Gabrielli 2022 ). SVT is not a presenting dysrhythmia consistent w/ ACS.
Other causes of sickling: acidosis, dehydration, inflammation, infection, fever, and blood stasis Sickling leads to vascular occlusion, end-organ ischemia, and decreased RBC lifespan, which, in turn, leads to pain crisis, acute anemia, sequestration, infection, and acute chest syndrome (ACS.) Each episode of ACS has a 9% mortality rate.
Sickling leads to vascular occlusion, end-organ ischemia, and decreased RBC lifespan, which, in turn, leads to pain crisis, acute anemia, sequestration, infection, and acute chest syndrome (ACS). ACS is lung injury due to vaso-occlusion in the pulmonary vasculature; many with ACS will have a concomitant vaso-occlusive pain crisis.
Date: June 30th, 2022 Reference: McGinnis et al. AEM June 2022. Date: June 30th, 2022 Reference: McGinnis et al. AEM June 2022. If we thought about ACS, we brought them in. AEM June 2022. Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter?
An expert committee appraised the evidence behind recommendations to avoid imaging to inform the 2022 NICE guidance. Each article will take a deeper dive into each recommendation’s supporting evidence and practical implications. The parents of 18-month-old Susie brought her to the Emergency Department after she had a seizure at home.
Date: May 24th, 2022 Reference: Broder et al. Date: May 24th, 2022 Reference: Broder et al. AEM May 2022 Guest Skeptic: Dr. Justin Morgenstern is an emergency physician and the creator of the #FOAMed project called First10EM.com Case: A 33-year-old male presents to the emergency department (ED) complaining of abdominal pain.
Smith : As Willy states, ACS with persistent symptoms is a guideline recommended indication for <2 hour angio (both ACC/AHA and ESC). Smith : As Willy states, ACS with persistent symptoms is a guideline recommended indication for <2 hour angio (both ACC/AHA and ESC). So I would be worried about inferior OMI. At midnight.
But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. Potassium was normal.
The patient was thought to have low likelihood of ACS, and cardiology recommended repeat troponin, urine drug testing, and echocardiogram. At that point, cardiology elected to treat for ACS. NOTE: For review of 20 cases of "Swirl" vs Swirl "Look-Alikes" — Check out the October 15, 2022 post in Dr. Smith's ECG Blog.
Morley 2022) This myth is: BUSTED. When you read the Morsel on Perichonditis of the ear last week ( or perhaps the Plantar Puncture Morsel from many many many weeks ago ) you may have objected because of the mention that, when indicated, fluroquinolones are safe in children. Which is a risk of 1 event for 62.5
You must understand this and the dynamic nature of ACS to provide excellent care for such patients. Comment by K EN G RAUER, MD ( 12/12 /2022 ): = I will summarize in 4 words the important message conveyed by Dr. Meyers in today's post = "Be Aware of Pseudo-Normalization!" This is termed " pseudo-normalization."
Accessed May 7, 2022. Background Crotalidae ovine polyvalent immune F(ab) (CroFab®) is the most widely available crotalid antivenom in the United States and is approved for severe crotalid envenomation with severe or progressive localized symptoms, systemic toxicity, and signs of hematologic toxicity on labs.
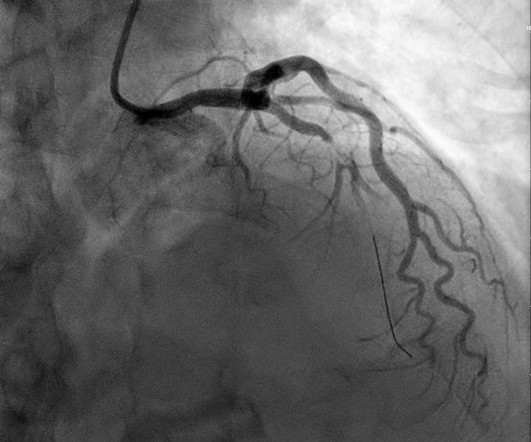
Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. It is not yet available, but this is your way to get on the list. link] Case continued She arrived in the ED and here is the first ED ECG.
Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1] Clin Cardiol 2022 4. 1] European guidelines add "regardless of biomarkers". But only 6.4% Int J Cardiol 2024 3. Lupu et al.
Ischemia from ACS causing the chest discomfort, with VT another consequence (or coincidence)? Cardioversion will address the rhythm problem immediately, also if the chest discomfort subsides when SR is restored, ischemia from ACS becomes much less likely. In either case, prompt cardioversion is indicated.
Episode 107: Eclampsia Definition: Severe hypertensive disease of pregnancy (HDP) with new onset tonic-clonic, focal, or multifocal seizures or unexplained altered mental status in a patient who is pregnant or postpartum and there’s no other causative etiologies. This is not borne out in the literature. The incidence is 1.5
He had no symptoms of ACS. His HEAR score (before troponin resulted) was documented at 3, with documentation stating "low suspicion for ACS." A troponin this high in a patient with no known chronic troponin elevation, and active acute ACS symptoms, has a very high likelihood of type 1 ACS regardless of the ECG.
And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! See this study showing an association between morphine and mortality in ACS: Use of Morphine in ACS is independently associated with mortality, at odds ratio of 1.4. Do NOT give it unless you are committed to the cath lab!!
At this point there are two large questions. #1. Am I missing anything? #2. What is this patient’s disposition? Pathophysiology and Etiology: In adults, sinus tachycardia is a heart rate greater than 100 beats per minute (bpm) originating from the sinoatrial (SA) node. This cardiac output increase is often due to need for increased oxygen delivery.
It is relieved with rest." == MY Comment, by K EN G RAUER, MD ( 11/1 /2022 ): == Like Dr. Smith — I interpreted the initial ECG in today’s case without the benefit of any history. He had been smoking an opiate and suddenly collapsed. He was ventilated with BVM on arrival. He awoke with naloxone. He denied any CP or SOB. It does not radiate.
Published 2022 Sep 2. ACS surgeons appeared to select surgery as their initial choice substantially more frequently than other subspecialties. ACS surgeons would have sent 6/43 patients for ERCP or MRCP (14%), whereas surgical oncologists would have sent a higher percentage of patients for ERCP or MRCP (7/18 or 38.9%).
In our opinion it should not be given in ACS unless you are committed to the cath lab. Learning Point: Any NSTEMI patient with active ongoing ACS symptoms refractory to medical management is supposed to go to the cath lab within 2 hours if available, per all guidelines in world, regardless of ECG findings. Published 2022 Feb 20.
Thus, this does NOT meet STEMI criteria (though, as of 2022, it is a formal "STEMI equivalent", assuming everyone agrees that this is de Winter morphology, for which there is currently no objective definition). Also, if you use the LAD OMI formula : QT = 420, RAV4 = 5 mm, QRSV2 = 6 mm, STE60V3 = 2.5 mm, the value is 22.2 (LAD What a farce.
More common in the setting of atherosclerotic lesions than emboli, which typically occur with sudden onset of symptoms. Symptoms may range from days to months prior to stroke onset. As many as two-thirds of patients with BAO experience prodromal symptoms, including TIAs, minor strokes, or other symptoms.
Smith: If this is ACS (a big if), t his is just the time when one should NOT use "upstream" dual anti-platelet therapy ("upstream" means in the ED before angiography). History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. Anything more on history?
2023 Apr 20:fetalneonatal-2022-324835. 2023 Apr 4:archdischild-2022-325281. De Alwis AC, et al. De Alwis AC, et al. We suggest this list can help you discover relevant or interesting articles for your local journal club or allow you to keep a finger on the pulse of paediatric research. Kuypers KLAM, et al. 2023 Apr 18.
You ask your anaesthetist to get ready to sedate or intubate depending on their status – Significant risk to the department – you make sure security is aware And your patient arrives. Ranulf is quite a sweet, round-faced boy, accompanied by his traumatised-looking mother as he is wheeled to your trauma bay.
For examples of this phenomenon — See My Comment in the February 14, 2018 — July 21, 2020 — and December 22, 2022 posts in Dr. Smith's ECG Blog ). The emergency physician was skeptical and believed the ECG to be a mimic, a false positive. So they looked into the patient's chart. Learning Point: 1. It is already approved in Europe.
NOTE: For more on “My Take” regarding a historical perspective, including current clinical relevance of recognizing Wellens' Syndrome — See My Comment at the bottom of the page of the August 12, 2022 post. Her symptoms were described as "pressure" with left arm radiation. No diaphoresis or vomiting. How to Check Your Findings.
Current can be alternating current (AC) or direct current (DC) with AC typically more dangerous as it is more likely to cause tetanic contractions and increase contact time with the electrical source. 2,3,5 Except for laundry or electrical car outlets (240 V AC), all U.S. household outlets are rated at 120 V AC.
If this is ACS with Aslanger's pattern , the ST depression vector of subendocardial ischemia (due to simultaneous 3 vessel or left main ACS) is directed toward lead II (inferior and lateral). Thus, this apparently is Aslanger's Pattern (inferior OMI with single lead STE in lead III, with simultaneous subendocardial ischemia).
MOREVER, the morphology of the TWI is just not right for ACS. showed that, when T-waves are inverted in precordial leads, if they are also inverted in lead III and V1, then pulmonary embolism is far more likely than ACS. Figure-2: ECG findings associated of acute PE ( reproduced from My Comment in the March 28, 2022 post ).
Assessing the Severity The severity of an electrical burn depends on several factors: the type of current (AC or DC), voltage, the pathway of the current through the body, the duration of contact, and the victim’s overall health. The entry and exit wounds are key indicators, but they can be small or hidden under clothing.
This is now further confirmation of ACS. The ACC/AHA guidelines mandate less than 2 hours cath for patients with ACS with refractory pain, pulmonary edema, or electrical or hemodynamic instability. Another ECG was recorded at 160 minutes: There is evolution, with worsening of ischemia. No wall motion abnormality.
Sepsis, hyperthyroidism, dehydration, heart failure, ACS, etc). However, digoxin is known for its rate-control properties and its direct vagal effect on the atrioventricular node. Paper: Mason JM, et al. Amiodarone versus digoxin for acute rate control of atrial fibrillation in the emergency department. Am J Emerg Med.
Clin Cardiol 2022; [link] Labs included: hsTnI 156 ng/L, Hb 12 g/dL, WBC 12x10^9/L, Cr. Smith comment: We have shown that use of opiates is associated with worse outcomes in ACS: Bracey, A. Opioids in ACS may reduce the pain score, but do not provide reperfusion for ongoing ACS. No history of GIB, dysuria, or GU symptoms.
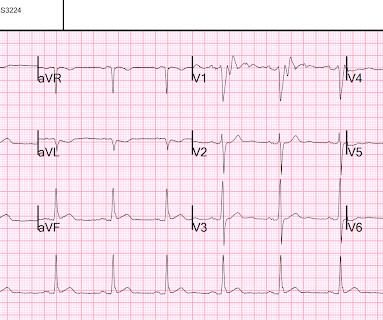
Considering hyperacute T-waves have been accepted as STEMI equivalents, it is possible that pseudonormalization could gain more recognition as an indicator of ACS. 2022 Nov, 80 (20) 1925–1960. Discussion The initial EKG performed demonstrated pseudonormalization of the T-wave in the presence of myocardial ischemia. J Am Coll Cardiol.
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chest pain. V1 has 0.5 mm of elevation. Learning Points: 1.
The ECG is diagnostic for acute transmural infarction of the anterior and lateral walls, with LAD OMI being the most likely cause (which has various potential etiologies for the actual cause of the acute coronary artery occlusion, the most common of which is of course type 1 ACS, plaque rupture with thrombotic occlusion).
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content