This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The person I was texting knows implicitly based on our experience together that I mean "Definite posterior OMI, assuming the patient's clinical presentation is consistent with ACS." The interventional cardiologist then canceled the activation and returned the patient to the ED without doing an angiogram ("Not a STEMI").
Cath lab declined as it is not a STEMI." And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! Another myocardial wall is sacrificed at the altar of the STEMI/NonSTEMI mindset. Do NOT give it unless you are committed to the cath lab!! Cath attending is aware. Abstract 556.
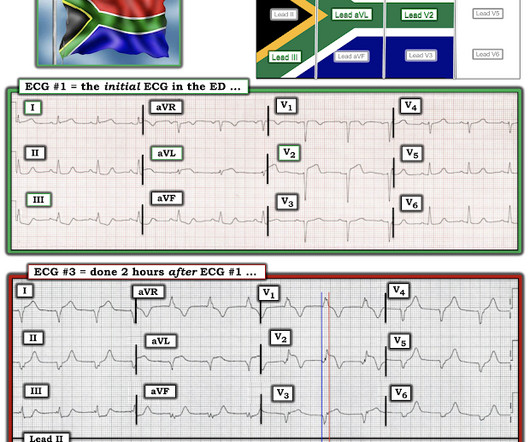
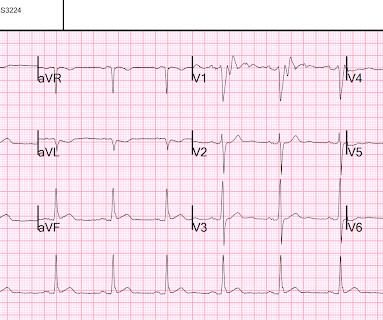
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. Review of the 2 ECGs in today's case is insightful ( Figure-1 ): The initial ECG shows sinus rhythm, LAHB and meets Peguero Criteria for LVH ( See My Comment in the August 15, 2022 post of Dr. Smith's ECG Blog for more on LVH criteria ).
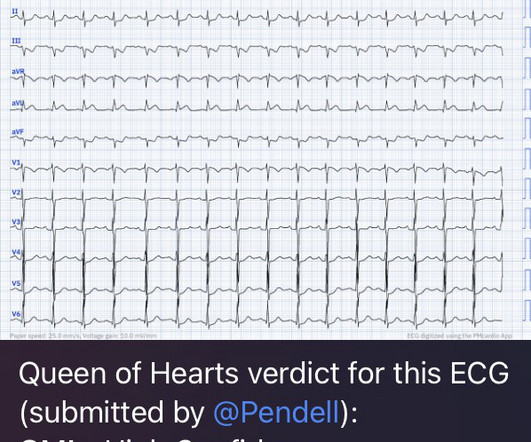
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." Smith : As Willy states, ACS with persistent symptoms is a guideline recommended indication for <2 hour angio (both ACC/AHA and ESC).
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. This is not unusual. Take home 1.
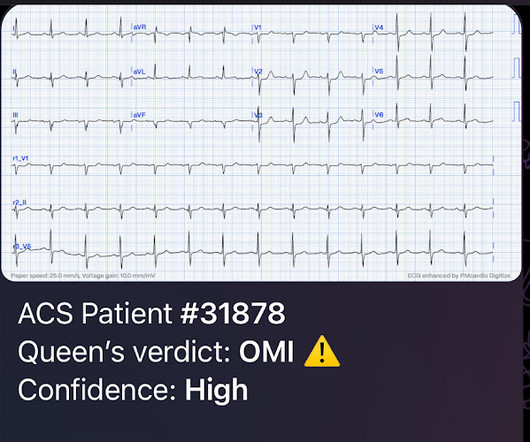
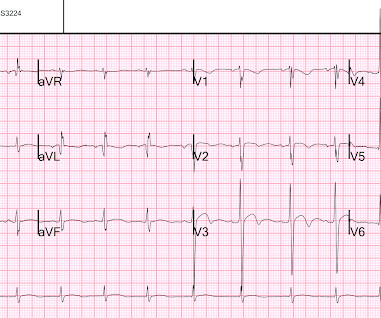
I sent this ECG to the Queen of Hearts (PMcardio OMI), and here is the verdict: You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form Then I learned that a Code STEMI was activated for concern of anterior "STEMI" in V1-V2. High sensitivity troponin I was 23 ng/L.
Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. This has resulted in an under-representation of STEMI MINOCA patients in the literature. From Gue at al.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. His response: “subendocardial ischemia. Anything more on history? POCUS will be helpful.”
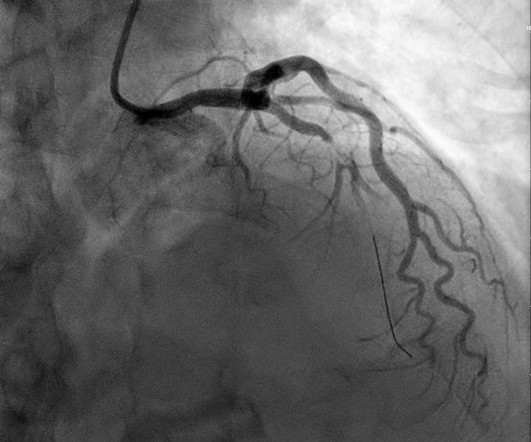
The cardiologists decided to overrule the STEMI criteria and the cath lab activation was NOT cancelled, and she was taken immediately to the cath lab and found to have an acute thrombotic distal LAD occlusion (TIMI 0). At triage she stated her pain is still persistent, but it is mildly improved compared to when she decided to come to the ED.
The ECG was read as "No STEMI" and the patient was treated like an average chest pain patient (despite the fact that a chest pain patient with active pain and active subendocardial ischemia is very high risk). In our opinion it should not be given in ACS unless you are committed to the cath lab. Published 2022 Feb 20.
Since then, I started looking for OMI EKG findings and not just STEMI. Remember: these findings above are included as STEMI equivalent findings in the 2022 ACC Expert Consensus Decision Pathway on ACS Patients in the ED. mm in lead I, thus not STEMI criteria) and was finally understood by the cardiologist.
The ECG is diagnostic for acute transmural infarction of the anterior and lateral walls, with LAD OMI being the most likely cause (which has various potential etiologies for the actual cause of the acute coronary artery occlusion, the most common of which is of course type 1 ACS, plaque rupture with thrombotic occlusion).
He had no symptoms of ACS. The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chest pain)? His HEAR score (before troponin resulted) was documented at 3, with documentation stating "low suspicion for ACS." Physician: "No STEMI."
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery.
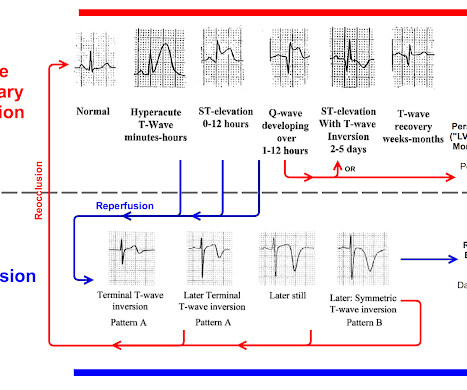
Considering hyperacute T-waves have been accepted as STEMI equivalents, it is possible that pseudonormalization could gain more recognition as an indicator of ACS. 2022 Nov, 80 (20) 1925–1960. 5 Studies looking at this phenomenon in the emergency department setting for patients presenting with chest pain are lacking.
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
Had the cardiologists followed NSTEMI or transient STEMI guidelines, which recommend non-urgent cath, the patient could have redeveloped an OMI and had a worse outcome. But this foresight will not be recorded, because the patient was diagnosed as "transient STEMI", even though no ECG ever met STEMI criteria. Take home 1.
Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. This was several months after the 2022 ACC Guidelines adding modified Sgarbossa criteria as a STEMI equivalent in ventricular paced rhythm). LAFB, atrial flutter, anterolateral STEMI(+) OMI. Limkakeng AT.
I knew that, if the patient had presented with chest discomfort, that this ECG is diagnostic of inferior posterior OMI, even though it is not a STEMI. This is now further confirmation of ACS. I was reading ECGs on the system, and saw this one: What do you think? There is no doubt that this is an inferior posterior OMI.
If this is ACS with Aslanger's pattern , the ST depression vector of subendocardial ischemia (due to simultaneous 3 vessel or left main ACS) is directed toward lead II (inferior and lateral). Thus, this apparently is Aslanger's Pattern (inferior OMI with single lead STE in lead III, with simultaneous subendocardial ischemia).
Immediate and early percutaneous coronary intervention in very high-risk and high-risk Non-STEMI patients. Clin Cardiol 2022; [link] Labs included: hsTnI 156 ng/L, Hb 12 g/dL, WBC 12x10^9/L, Cr. Smith comment: We have shown that use of opiates is associated with worse outcomes in ACS: Bracey, A. Lupu L, et al. mg/dL, K 3.5
You must understand this and the dynamic nature of ACS to provide excellent care for such patients. Comment by K EN G RAUER, MD ( 12/12 /2022 ): = I will summarize in 4 words the important message conveyed by Dr. Meyers in today's post = "Be Aware of Pseudo-Normalization!"
Later, she developed chest pain again, and had this ECG recorded: Obvious Anterior OMI that is also a STEMI Coronary angiogram- --Right dominant coronary artery system --The left main artery was normal in appearance and free of obstructive disease. --The Thus, Wellens' syndrome should be thought of as a transient OMI or transient STEMI.
Corroborating this is the subtle ST depression in V2-V3 which is inappropriate for the normal QRS complex, and in the context of ACS, we have shown this is quite specific for posterior OMI. In the context of ACS, ST depression maximal in V1-V4 (rather than V5-V6) not due to a QRS abnormality is specific for posterior OMI.
Discharge Diagnosis was STEMI (The STE did not meet "criteria," so "OMI" would be better, but "STEMI" is far better than what this could have been called: NonSTEMI) Quotes from a note written by a really fine and knowledgable physician: "12-lead EKG was obtained initial 1 at time zero. Chest pain is squeezing or tight in nature.
It was shown to me with worry for ischemic ST elevation, which is certainly possible from severe CO toxicity, or concomitant ACS. Intravascular Neutrophil Activation Due to Carbon Monoxide Poisoning What do you think of this ECG? Routine ECG recorded before hyperbaric therapy.Are they related?
But it doesn’t meet STEMI criteria, and was not identified by the computer or the over-reading cardiologist. The emergency physician wasn’t sure what to make of the changes from one ECG to the next but was concerned about ACS. Still no WPW pattern, and more obvious inferoposterior OMI, but still STEMI negative. CMAJ 2014.
Recall that, in the setting of ACS symptoms, ST depression that are maximal in leads V1-V4 (as opposed to V5 and V6) not attributable to an abnormal QRS complex is specific for OMI. Close up of V3 with baseline in red Close up of V4 with baseline in red This ECG alone is highly suspicious for posterior OMI!
ST depression maximal in V1-V4, in the context of ACS symptoms and unexplained by QRS abnormality or tachydysrhythmia, should be considered posterior OMI until proven otherwise.
2022 Mar; 17. 2022 Mar; 17. PMID: 30060961 Koller AC, et al. As above, we take the PCAC score into account when we order our interventions and may prioritize Neuroresuscitation in a PCAC 4 over a cath without a hard indication (STEMI). Paper: Nassal MMJ, et al. Resuscitation. REFERENCES: Nassal MMJ, et al. Resuscitation.
STEMI negative : the EMS automated interpretation read, “STEMI negative. According to the STEMI paradigm, the patient doesn’t have an acute coronary occlusion and doesn't need emergent reperfusion, so the paramedics can bring them to the ED for assessment, without involving cardiologists. Inferior infarct, age undetermined.
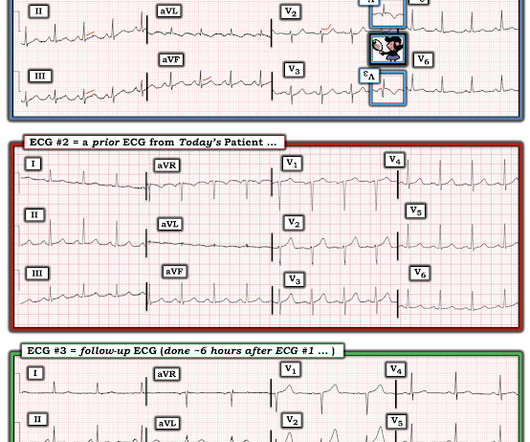
He has a history of coronary artery disease and a STEMI two years prior that was treated with primary PCI. At the time of this initial ED ECG, his symptoms were improving ECG #1 on admission to the ED The patient was not seen quickly in the ED as it was a busy shift and the ECG did not meet STEMI criteria. The below ECG was recorded.
Acute coronary syndrome (ACS), cardiomyopathy, cardiogenic shock, aortic dissection, pulmonary embolism, myocarditis/pericarditis, cardiac tamponade, coronary artery dissection, coronary vasospasm, ventricular aneurysm What are your next steps in management for this patient? Consider serial EKGs, which may demonstrate evolution of disease.
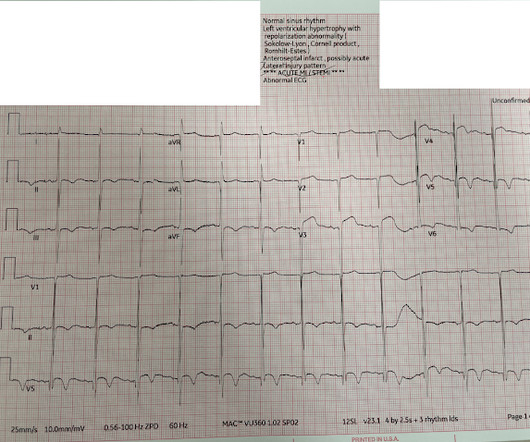
Even before we have clinical context, this ECG simply does not appear concerning for OMI, notwithstanding the machine's interpretation ** ** ACUTE MI / STEMI ** **. But in the world of STEMI, this is a challenging ECG to most. When the Queen has some suspicion of OMI, she asks if the patient has ACS Symptoms.
This dynamic change is diagnostic of ACS. Cardiology was consulted and agreed that his history was high risk for ACS and a next-day angiogram was merited. This was also non-diagnostic for OMI, although the dynamic changes are diagnostic of ACS. ECG at time 82 minutes: What do you think?
Here is the prehospital ECG, recorded in the presence of pain: Hyperacute anterolateral STEMI The medics had activated the cath lab and the patient went for angiogram and had a 95% stenotic LAD with TIMI-3 flow. So even a massive STEMI, if it reperfused quickly, can result in a relatvely low troponin (in contrast to the next case!)
Summary : it is hard to say whether this ST Elevation was initiated by 1) something which led to pulmonary edema, then hypoxia, then supply-demand mismatch, or 2) whether ACS with OMI combined with some other pre-existing condition led to a decrease in LV function and pulmonary edema. Also see these posts of Type II STEMI. Management?
Negative trops and negative angiogram does not rule out coronary ischemia or ACS. It is correct that he did not have chest pain, but we must remember that fully 1/3 of full blown STEMI do not present with chest pain. This is extremely elevated for a type 2 MI and totally consistent with STEMI. See these posts: Dynamic OMI ECG.
After completing the ACS algorithm with amiodarone and lidocaine, there are diminishing returns on further treatments. Or was it out of proportion, perhaps worsened by the sympathetic surge? We will never know for certain. In addition to profound acute heart failure, the patient suffered from electrical storm. link] Bai, J., Tang, Z., &
50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). Patients with suspected ACS should be evaluated with echocardiography. This correlates with potentially salvageable myocardium. See Raitt et al.:
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content