This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Date: June 30th, 2022 Reference: McGinnis et al. AEM June 2022. Date: June 30th, 2022 Reference: McGinnis et al. AEM June 2022. Reference: McGinnis et al. AEM June 2022. Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter?
EBM Update: Steroids in Severe CAP and CT in Post ROSC OHCA #1: Dequin PF, Meziani F, Quenot JP, et al; CRICS-TriGGERSep Network. 2022 Aug;48(8):1009-1023. Author Takeaway: No difference in mortality at 60 days with methylprednisolone vs. placebo in severe CAP #3: Wu JY, Tsai YW, Hsu WH, et al. N Engl J Med. Intensive Care Med.
American Gastroenterological Association issued a practice guideline in November 2022 recommending that semaglutide 2.4 Retrospective study published in 2022 of 81,752 adverse events associated with GLP-1 agonist therapy found an increased risk of pancreatitis, particularly with liraglutide (ROR 32.67; 95% CI 29.44-36.25).
Similarly, if a patient with known CAD presents with refractory ischemic chest pain, the ECG barely matters: the pre-test likelihood of acute coronary occlusion is so high that they need an emergent angiogram. Amsterdam et al. Alencar et al. Lupu et al. Clin Cardiol 2022 4. Herman, Meyers, Smith et al.
The patient proceeded to cath where all coronaries were described as normal with no evidence of any CAD, spasm, or any other abnormality. In the largest study looking at this topic by Mizusawa et al., Recently the rate of true arrhythmic events related to fevers in the classic Brugada Type 1 syndrome was explored by Michowitz et al.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. Hayakawa A, Tsukahara K, Miyagawa S, et al. Published 2022 Feb 20. 2022;Available from: [link] 7. Am J Emerg Med.
Late Gadolinium enhancement: Multifocal scarring of the septum (including RV septum), basal anterior wall and transmural mid inferior region scarring - a non-CAD hyperenhacement pattern. For review of a case of RVOT VT — Please see My Comment at the bottom of the page in the February 14, 2022 post in Dr. Smith's ECG Blog.
Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al. J Electrocardiol [Internet] 2022;Available from: [link] Cardiology opinion: Takotsubo Cardiomyopathy (EF 30-35%) V Fib Cardiac arrest Prolonged QTC NSTEMI (Smith comment: is it NSTEMI or is it Takotsubo? Lindahl et al. From Gue at al.
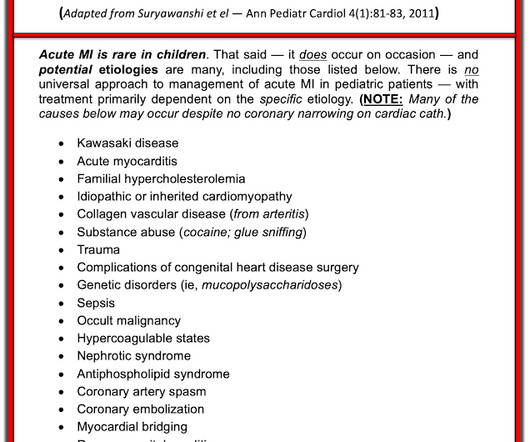
He did have a family history notable for early CAD. hematological disorder like sickle cell or antiphospholipid syndome, family history of CAD or hypercholesterolemia, prior history of vasculopathies such as Kawasaki Disease, MIS-C, prior cardiac surgery, etc.) He denied drug or alcohol use. mg/L and a normal WBC of 8.8. .-
He has a history of CHF, dilated cardiomyopathy, HTN, HLD and CAD. Isenhour JL, Craig S, Gibbs M, et al. For this box, please keep ventricular tachycardia (VTach) and supraventricular tachycardia with aberrancy (SVT with aberrancy) in your differential. This EKG comes from a 75-year-old male presenting with palpitations. Vereckei A.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














Let's personalize your content