This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
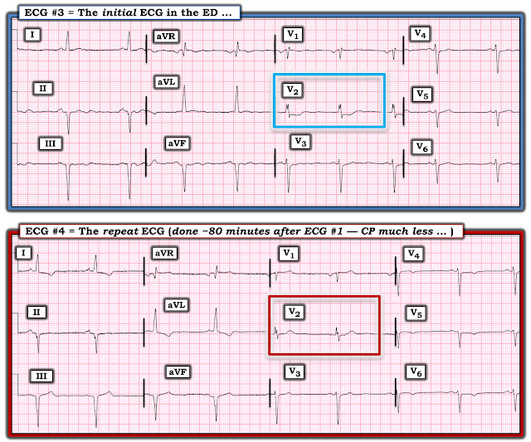
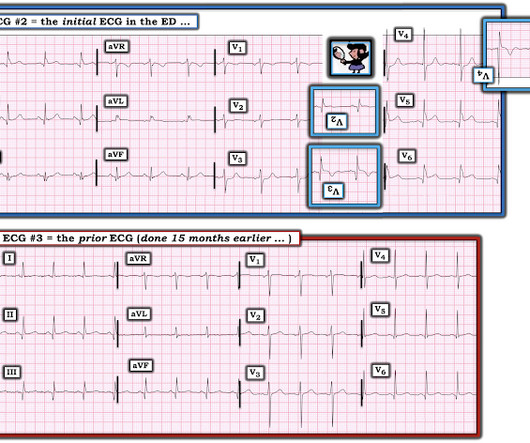
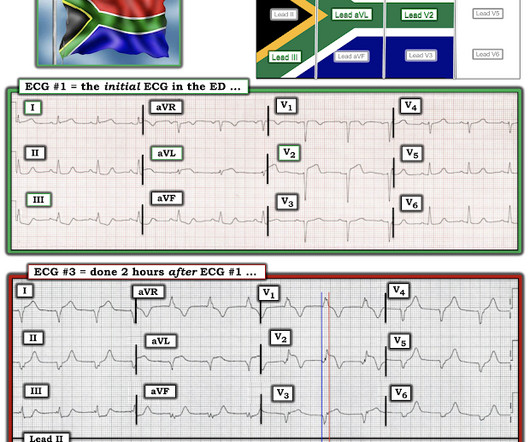
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. Here is his most recent previous ECG: This was recorded after intervention for inferior STEMI (with massive ST Elevation, see below), and shows inferior Q-waves with T-wave inversion typical of completed inferior OMI. ng/mL (quite large).
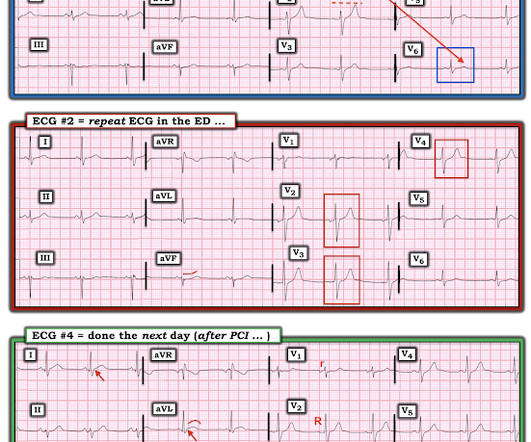
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
Cath lab declined as it is not a STEMI." And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! Another myocardial wall is sacrificed at the altar of the STEMI/NonSTEMI mindset. de Winter et al in N Engl J Med 359:2071-2073, 2008. Cath attending is aware. Abstract 556.
Date: February 1, 2023 Reference: Wolfrum et al. September 2022 Guest Skeptic: Dr. Justin Morgenstern is an emergency physician and the creator of the #FOAMed project called www.First10EM.com Case: You are working an overnight shift at a small rural hospital. Date: February 1, 2023 Reference: Wolfrum et al. Circulation.
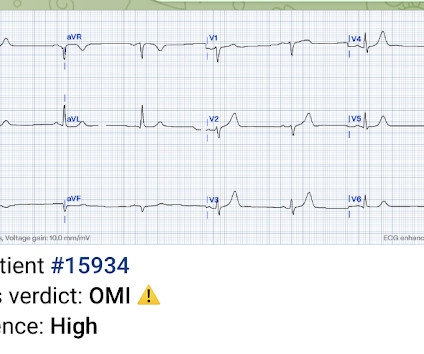
This was a machine read STEMI positive OMI. 118.007305) from Heitner et al. , The meaning of this quote is that at times, something as obvious as the dramatic anterior lead ST elevation that we see in today's tracing is not the result of an acute LAD STEMI. His ECG is shown below. Pretty obvious anterior current of injury.
Smith’s ECG Blog has published a growing list of over 40 cases of ECGs falsely labeled ‘normal’ by the computer which are diagnostic of Occlusion MI, and Smith et al. This is diagnostic of LAD occlusion but is equivocal for STEMI criteria and was missed (and both labeled ‘normal’ by final cardiology interpretation).
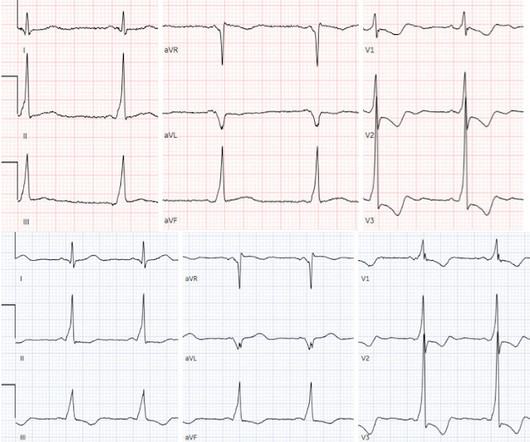
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. Herzog et al. Khan et al. Circulation 2007 2.
The latest is Langlois-Carbonneau et al. If we took this as the gold standard, we would conclude that the computer interpretation was safe and accurate at least accurate enough to not miss STEMI, and that physicians should not be interrupted to interpret it, because there would be no change in patient management.
Unknown algorithm The Queen gets it right Case 4 How unreliable are computer algorithms in the Diagnosis of STEMI? The patient's prehospital ECG showed that there was massive STEMI and these are hyperacute T-waves "on the way down" as they normalize. Pain was resolving. Diagnosed as Normal by the computer. Troponin negative.
Lindahl et al. From Gue at al. STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. This has resulted in an under-representation of STEMI MINOCA patients in the literature. References: 1.
Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). As far as I can tell, there is only one randomized trial of immediate vs. delayed intervention for transient STEMI. Lemkes JS, et al.
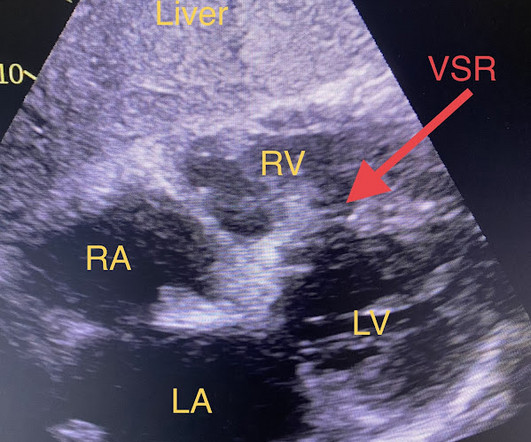
The conventional machine algorithm interpreted this ECG as STEMI. See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI. She was out walking her dog when she developed sudden dizziness and light-headedness. When EMS found her, she was dyspneic and diaphoretic.
The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. The paramedic notes called STEMI into question: “EMS disagree with monitor for STEMI callout. Vitals were normal except for oxygen saturation of 94%. Vitals were normal.
A Short Comment on PIRP and T Waves: Oliva et al found a strong association of myocardial rupture with postinfarction regional pericarditis. It has been estimated that in the aggregate, they occur at a rate of about 3 per 1000 patients with acute MI, and most of these events occur in patients with STEMI.
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. Studies such as those by Moise et al 14 and Ellis et al 39 have shown that the relative risk of developing an acute myocardial infarction in the territory supplied by an artery with a 70%. He was started on nitro gtt.
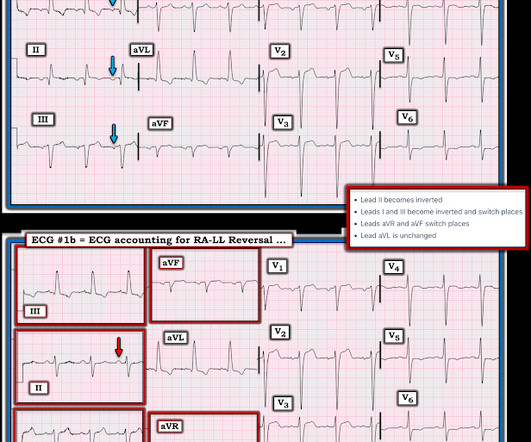
Here, I do not see OMI (although the ECG is falsely STEMI positive with just over 1 mm STE in V1 and about 2.5 The April 17, 2022 post ( Leads V1,V2 misplacement ). The May 5, 2022 post ( LA-RA reversal ). The May 24, 2022 post ( LA-LL reversal ). The May 26, 2022 post ( LA-LL reversal ). What do you think?
So we activated the Cath Lab Angiogram: Impression and Recommendations: Culprit for the patient's anterior ST segment myocardial infarction and out of hospital V-fib cardiac arrest is a thrombotic occlusion of the mid LAD The first troponin returned barely elevated at 36 ng/L (URL = 35) In our study of initial troponin in STEMI, 26.8%
But because there was no new ST elevation, the ECG was signed off as “STEMI negative” and the patient waited to be seen. But the ECG still doesn’t meet STEMI criteria. It was therefore interpreted as “no STEMI” and the patient was treated with dual anti-platelets and referred to cardiology as “NSTEMI.” the cardiologist 5.
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. Harhash AA, Huang JJ, Reddy S, et al. aVR ST segment elevation: acute STEMI or not?
The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chest pain)? Physician interpretation: "No STEMI." Physician: "No STEMI." Cardiologist interpretation: "Technically does not meet STEMI criteria but concerning for ischemia."
Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al. J Electrocardiol [Internet] 2022;Available from: [link] Cardiology opinion: Takotsubo Cardiomyopathy (EF 30-35%) V Fib Cardiac arrest Prolonged QTC NSTEMI (Smith comment: is it NSTEMI or is it Takotsubo? Lindahl et al. From Gue at al.
4 Formerly, chest pain patients without an S-T Elevation Acute Myocardial Infarction (STEMI), whose pain was suspected to be cardiac in nature, became inpatients for sequential monitoring of their lactate dehydrogenase and creatine kinase isozyme profiles. Updated September 21, 2022. February 22, 2022. Gulati M, et al.
Considering hyperacute T-waves have been accepted as STEMI equivalents, it is possible that pseudonormalization could gain more recognition as an indicator of ACS. 2022 Nov, 80 (20) 1925–1960. 5 Studies looking at this phenomenon in the emergency department setting for patients presenting with chest pain are lacking. J Am Coll Cardiol.
The ECG was read as "No STEMI" and the patient was treated like an average chest pain patient (despite the fact that a chest pain patient with active pain and active subendocardial ischemia is very high risk). Hayakawa A, Tsukahara K, Miyagawa S, et al. Published 2022 Feb 20. 2022;Available from: [link] 7. Am J Emerg Med.
This is guideline approved by both ACC/AHA and by European guidelines. == Comment by K EN G RAUER, MD ( 6/1/2022 ): == I found serial evaluation of sequential tracings in today's case to be subtle — yet highly insightful. A patient with active chest pain and an otherwise unexplained elevated troponin should go to the cath lab.
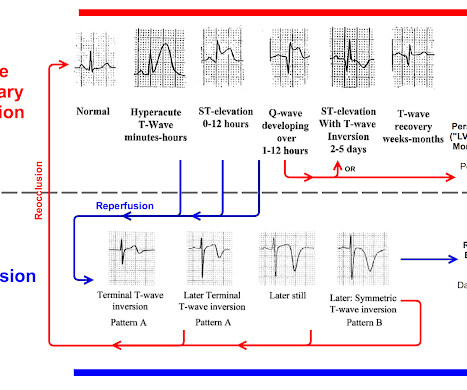
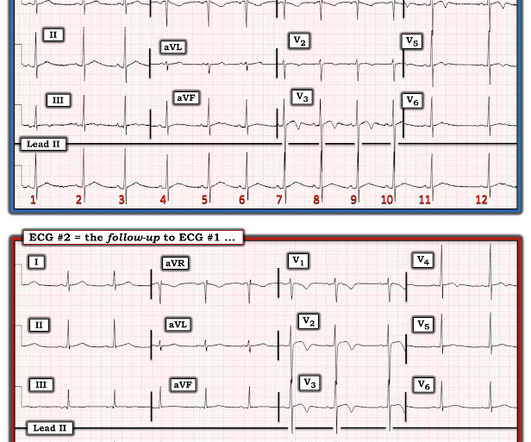
While this ECG is negative for “posterior STEMI”, the resolution of anterior ST depression (accompanied by the troponin elevation) confirms posterior OMI with spontaneous reperfusion. The second opportunity to make the diagnosis and expedite angiography was missed because the ECG never met STEMI criteria and continued to be labeled ‘normal.’
The HEART and EDACS scores are helpful to risk stratify patients with chest pain, but they hinge on accurate ECG interpretation: a low score doesn’t apply if the ECG shows STEMI(+)OMI, and shouldn’t be used for STEMI(-)OMI or OMI reperfusion either 2. Backus BE, Six AJ, Kelder JC, et al. Moumneh T, Sun BC, Baecker A, et al.
Meyers, Bracey, Smith, et al. OMI that are not STEMI can be very subtle and difficult to diagnose even though the findings are very specific. With a little bit of practice — it becomes EASY to recognize the "shelf-like" ( flat ) shape of ST depression — that looks like a stemi when this image is inverted. Learning Points.
There is clearly sufficient STE for STEMI criteria in leads V2 and aVL, but lead I has less than 1.0 mm of STE - thus, technically this ECG does not meet STEMI criteria, although it is a quite obvious OMI. This ECG was immediatel y discussed with the on-call cardiologist who said the ECG was "concerning but not a STEMI."
Here is the repeat ECG at 52 minutes after arrival to triage: Obvious posterolateral STEMI Angiographic findings: 1. Reference: • Writing Committee, Kontos MC, de Lemos JA, et al. Comparison of the ST-Elevation Myocardial Infarction (STEMI) vs. NSTEMI and Occlusion MI (OMI) vs. NOMI Paradigms of Acute MI. Meyers HP, Smith SW.
Comment by K EN G RAUER, MD ( 12/12 /2022 ): = I will summarize in 4 words the important message conveyed by Dr. Meyers in today's post = "Be Aware of Pseudo-Normalization!" Failure to do so may result in overlooking subtle ST-T wave changes in a patient "in passage" from a frank STEMI toward reperfusion changes.
The Cardiorespiratory Implications of Ultra-marathon Bjørkavoll‐Bergseth et al. Paana et al. Anterior STEMI? Please see My Comment at the bottom of the page in the April 17, 2022 post of Dr. Smith's Blog — for concise review on how to quickly recognize too-high placement of the lead V1 and V2 electrodes.
Smith and Meyers to diagnose both obvious (STEMI) and subtle OMI. We've previously discussed the all-too-often ignored entity known as MINOCA ( = MI with N on- O bstructive C oronary A rteries ) — which we detailed in the November 30, 2022 post in Dr. Smith's ECG Blog ( See My Comment at the bottom of the page ). It was trained by Drs.
But it doesn’t meet STEMI criteria, and was not identified by the computer or the over-reading cardiologist. Still no WPW pattern, and more obvious inferoposterior OMI, but still STEMI negative. Rosner et al. The emergency physician wasn’t sure what to make of the changes from one ECG to the next but was concerned about ACS.
If you still have not read it, I strongly recommend that you read the following article on the diagnosis of "posterior" MI: Ischemic ST-Segment Depression Maximal in V1-V4 (Versus V5-V6) of Any Amplitude Is Specific for Occlusion Myocardial Infarction (Versus Nonocclusive Ischemia), by Meyers HP et al. 2022 Mar-Apr;71:44-46.
Yelken B et al. With this ECG: See this typical case of cO poisoning: What is the treatment for this subendocardial ischemia? == MY Comment, by K EN G RAUER, MD ( 2/18 /2022 ): == Insightful case presented by Dr. Smith of this young adult who presented with accidental CO poisoning.
Lupu L, et al. Immediate and early percutaneous coronary intervention in very high-risk and high-risk Non-STEMI patients. Clin Cardiol 2022; [link] Labs included: hsTnI 156 ng/L, Hb 12 g/dL, WBC 12x10^9/L, Cr. Unfortunately, they follow their own guidelines only 6% of the time!! mg/dL, K 3.5
The limb leads have been removed because there was no ST elevation in those leads, the QRS complexes have been obscured because this is irrelevant to STEMI criteria, and red lines have been added to measure ST segment elevation. But STEMI criteria ignore all this and look at ST segments in isolation.
STEMI negative : the EMS automated interpretation read, “STEMI negative. According to the STEMI paradigm, the patient doesn’t have an acute coronary occlusion and doesn't need emergent reperfusion, so the paramedics can bring them to the ED for assessment, without involving cardiologists. Inferior infarct, age undetermined.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. In such cases — radiofrequency ablation of ectopic beats triggering malignant ventricular arrhythmias was needed for control of arrhythmic storm because the antiarrhythmic medications tried were ineffective ( Marrouche et al — JACC 5;43(9): 1715-20, 2004 ).
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content