This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Date: June 30th, 2022 Reference: McGinnis et al. Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? AEM June 2022. Date: June 30th, 2022 Reference: McGinnis et al. Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter?
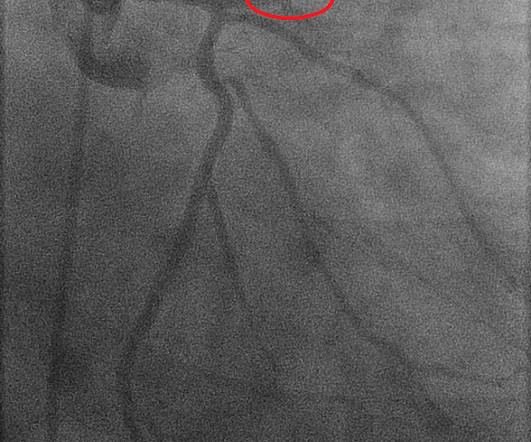
The patient was treated as possible NSTEMI and underwent coronary angiography about 4 hours after presentation. TIMI 3 means the rate of passage of dye through the coronary artery is normal by angiography.) Initial hsTnI was 384 ng/L. The report describes a 60% proximal LAD lesion with TIMI 3 flow.
The ECG is just a test: a Bayesian approach to acute coronary occlusion If a patient with a recent femur fracture has sudden onset of pleuritic chest pain, shortness of breath, and hemoptysis, the D-dimer doesn’t matter: the patient’s pre-test likelihood for PE is so high that they need a CT. Clin Cardiol 2022 4. Amsterdam et al.
A CT Coronary angiogram was ordered. Here are the results: --Minimally obstructive coronary artery disease. --LAD CAD-RADS category 1. --No Although a lesion is not visible anatomically on this CT scan, coronary catheter angiography could be considered based on Cardiology evaluation." A repeat troponin returned at 0.45
American Gastroenterological Association issued a practice guideline in November 2022 recommending that semaglutide 2.4 GLP-1 agonists are also associated with improved ejection fraction, coronary blood flow, and cardiac output while reducing the risk of cardiovascular events, infarction size, and all-cause mortality. How do they work?
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. The De Winter ECG pattern: morphology and accuracy for diagnosing acute coronary occlusion: systematic review. 2009;95:1701–1706.
Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy. Just because you don't see hemodynamically significant CAD on angiogram does not mean it is not OMI. It can only be seen by IVUS.
The patient proceeded to cath where all coronaries were described as normal with no evidence of any CAD, spasm, or any other abnormality. She has not had a heart catheterization or after this event so the presence or absence of CAD is still unknown.
The ED provider ordered a coronary CT scan to assess the patient for CAD. The patient was taken emergently to the cath lab for a pericardiocentesis instead of a coronary angiogram. Three months prior to this presentation, he received a pacemaker for severe bradycardia and syncope due to sinus node dysfunction.
As in all ischemia interpretations with OMI findings, the findings can be due to type 1 AMI (example: acute coronary plaque rupture and thrombosis) or type 2 AMI (with or without fixed CAD, with severe regional supply/demand mismatch essentially equaling zero blood flow). This patient arrested shortly after hospital arrival.
Late Gadolinium enhancement: Multifocal scarring of the septum (including RV septum), basal anterior wall and transmural mid inferior region scarring - a non-CAD hyperenhacement pattern. For review of a case of RVOT VT — Please see My Comment at the bottom of the page in the February 14, 2022 post in Dr. Smith's ECG Blog.
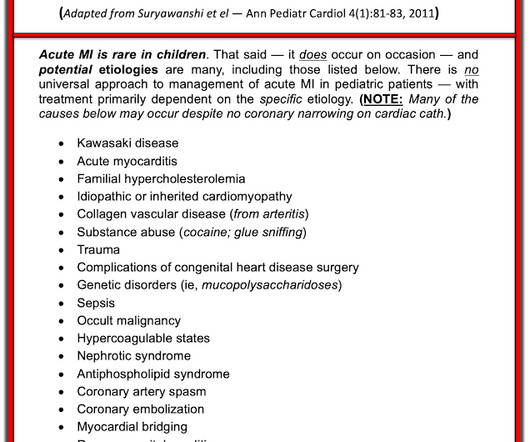
Acute coronary syndrome in a pediatric patient? He did have a family history notable for early CAD. hematological disorder like sickle cell or antiphospholipid syndome, family history of CAD or hypercholesterolemia, prior history of vasculopathies such as Kawasaki Disease, MIS-C, prior cardiac surgery, etc.)
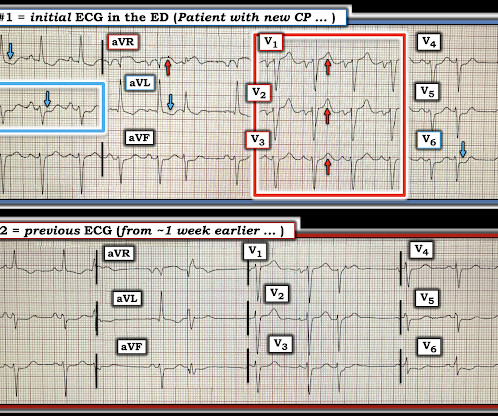
Hi Steve wonder what you think of this ecg in a 60 yo woman w cp, known CAD" Presentation ECG (ECG 1): Here is her previous from one week prior when she presented with heart failure and trops were "negative" (ECG 2): My response: "They both look like active ischemia. Figure-1: Comparison between the first 2 ECGs in today's case.
Written by Willy Frick A 52 year old man with hypertension, dyslipidemia, and seropositive rheumatoid arthritis (a risk factor for CAD) presented with acute substernal chest pressure with diaphoresis which woke him from sleep just after midnight. Smith and Meyers present 20 cases of "Swirl" or Swirl "look-alikes" in the October 15, 2022 post.
A 70-something dialysis patient presented and coronary disease had missed dialysis and then presented with acute onset of shortness of breath. Negative trops and negative angiogram does not rule out coronary ischemia or ACS. These features are most likely the result of significant underlying coronary disease. The dye don't lie".except
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content