This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
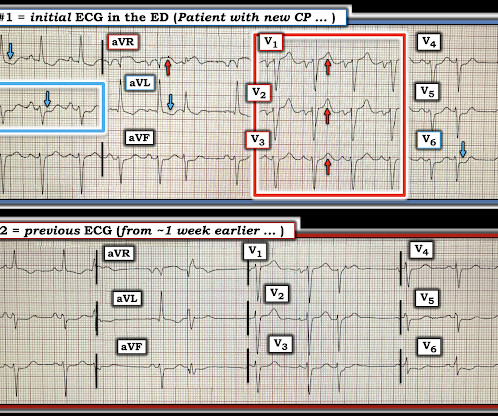
Date: June 30th, 2022 Reference: McGinnis et al. AEM June 2022. Date: June 30th, 2022 Reference: McGinnis et al. AEM June 2022. Case: You are working a shift in your local community emergency department (ED) when a 47-year-old male presents with chest pain. He is also the CME editor for Academic Emergency Medicine.
Despite otherwise normal vital signs, she was appropriately triaged to the critical care area of the ED. They are rare and hard to find in normal practice in the ED. For review of a case of RVOT VT — Please see My Comment at the bottom of the page in the February 14, 2022 post in Dr. Smith's ECG Blog. RVEF 100 ml/m2.
2022 Aug;48(8):1009-1023. Reyes LF, Garcia E, Ibáñez-Prada ED, et al. Low-dose methylprednisolone treatment in critically ill patients with severe community-acquired pneumonia. Intensive Care Med. Question: In adult patients admitted to the ICU with severe CAP, does methylprednisolone compared to placebo reduce 60-day all-cause?
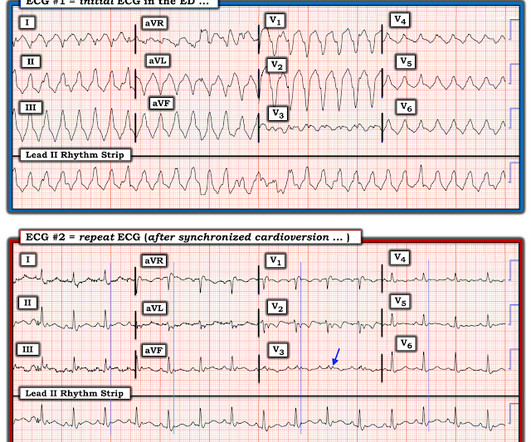
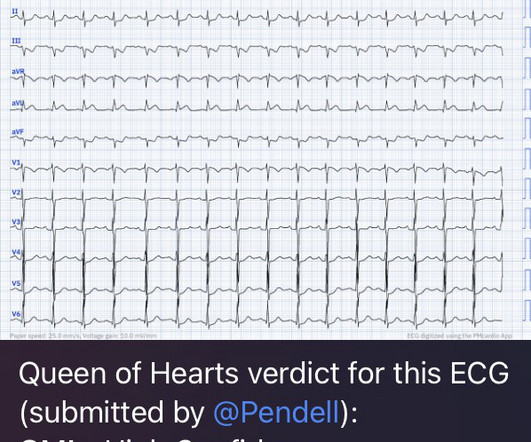
An ECG was performed in the ED at 1554: Original image unavailable, this is the only recorded scanned ECG available. QOH Interpretation: The initial troponin I (older generation) at the first ED was barely positive at 0.06 She has not had a heart catheterization or after this event so the presence or absence of CAD is still unknown.
Case An 82 year old man with a history of hypertension presented to the ED with chest pain at 1211. The ED provider ordered a coronary CT scan to assess the patient for CAD. His pain suddenly became much worse in the ED and he became acutely diaphoretic, dizzy, and hypotensive. Another blood pressure was checked.
Case "Male, 43yo, come to ED with Epigastric Pain started 3 hours ago. Remember: these findings above are included as STEMI equivalent findings in the 2022 ACC Expert Consensus Decision Pathway on ACS Patients in the ED. Since then, I started looking for OMI EKG findings and not just STEMI. Risk Factors: High Cholesterol.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. Published 2022 Feb 20. 2022;Available from: [link] 7. Hayakawa A, Tsukahara K, Miyagawa S, et al. J Cardiol Cases.
He reportedly told his family "I think I'm having a heart attack", then they immediately drove him to the ED, and he was able to ambulate into the triage area before he collapsed and became unresponsive. The value of Stat Echo in the ED for confirming clinical and ECG suspicion of acute PE cannot be overstated!
CAD-RADS category 1. --No That said — I did not feel the history we were given pointed to any particular diagnosis ( ie, 3 episodes of CP and dyspnea of uncertain duration over the past day — with pain on deep breathing — but with symptoms apparently resolved by the time the patient arrived in the ED ).
J Electrocardiol [Internet] 2022;Available from: [link] Cardiology opinion: Takotsubo Cardiomyopathy (EF 30-35%) V Fib Cardiac arrest Prolonged QTC NSTEMI (Smith comment: is it NSTEMI or is it Takotsubo? -- these are entirely different) Moderate single-vessel CAD. I could have told you this (and did tell you this) without an MRI.
He did have a family history notable for early CAD. An ECG was perfomed on arrival to our ED: NSR with ST elevation II,III, aVF with reciprocal depression in aVL Would you refer this pediatric patient for emergent PCI? He denied drug or alcohol use. The workup at the transferring hospital yielded elevated troponin I at 18.1
He has a history of CHF, dilated cardiomyopathy, HTN, HLD and CAD. Remember, from the ED point of view, if you are confronted with a wide complex regular tachydysrhythmia, assume VTach until proven otherwise! This EKG comes from a 75-year-old male presenting with palpitations. Take a look: Figure 3. Did you read it? Vereckei A.
This 60-year old woman clearly presented to the ED as a higher -risk patient given her history of known coronary disease, now with new chest pain. This was sent to me by a former resident who is outstanding at reading ECGs for OMI. "Hi
Written by Willy Frick A 52 year old man with hypertension, dyslipidemia, and seropositive rheumatoid arthritis (a risk factor for CAD) presented with acute substernal chest pressure with diaphoresis which woke him from sleep just after midnight. Smith and Meyers present 20 cases of "Swirl" or Swirl "look-alikes" in the October 15, 2022 post.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















Let's personalize your content