This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The 2022 American College of Cardiology (ACC) pathway provides timely guidance [1]. Intermediate-risk patients may be further stratified based on recent stress testing or coronary angiogram findings plus a modified HEART or Emergency Department Assessment of Chest Pain (EDACS) score. Time to know your hs-cTn better.
Compensatory enlargement was defined as being present when the total coronary arterial cross-sectional area at the stenotic site was greater than that at the proximal nonstenotic site. Thus, the lumen observed may actually still be the same size as the original, normal lumen. Unfortunately, vascular remodeling is variable and inconsistent.
Note that as many as 7% of patients with acute coronary syndrome have chest pain reproducible on palpation [Lee, Solomon]. which reduces the pre-test probability of acute coronary syndrome by less than 30% [McGee]. Chest pain reproducible on palpation does not rule out acute coronary syndrome. Guagliumi, G., Iwaoka, R.
Date: June 30th, 2022 Reference: McGinnis et al. Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? AEM June 2022. Date: June 30th, 2022 Reference: McGinnis et al. Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter?
Additionally, his cardiac telemetry monitor showed runs of accelerated idioventricular rhythm, a benign arrhythmia often associated with coronary reperfusion. The patient is a 75-year old man with known coronary disease, including prior LAD and LCx OMI. That this patient has severe underlying coronary disease is indisputable.
What Your Gut Says: The patient has a tachydysrhythmia which may be the presentation of acute coronary syndrome (ACS) even though the patient has no ischemic symptoms. Up to 80% of patients will have at least one troponin sent ( Gabrielli 2022 ). Type 2: MI secondary to ischaemia, but not related to coronary atherosclerosis.
” – Musings of an American ED resident in July 2022 when US healthcare was affected simultaneously by supply chain issues from GE Healthcare (contrast media) and Abbott Laboratories (Similac baby formula). A baby formula milk shortage for adults.” 11 Table 1.
Extracorporeal membrane oxygenation Of patients with out-of-hospital cardiac arrest presenting to the ED in refractory VF, a majority have significant coronary artery disease, much of which is amenable to percutaneous coronary intervention. Out-of-hospital cardiac arrest is a commonly encountered entity in U.S.
But like many similar studies, the study was small (one year at one centre with no indication of the incidence of acute coronary occlusion), and it used as the gold standard the final cardiologist interpretation of the ECG - not the patient outcome! 2022 ; 51 : 384 - 387. Smith comment: this is even more stupid. Take home 1.
Emergency physicians have recognized for some time that there are many occlusions of the coronary arteries that do not present with classic STEMI criteria on the ECG. In October 2022, the American College of Cardiology released an updated expert consensus decision regarding the evaluation of chest pain in the emergency department.
A 50-year-old Caucasian female with a history of hypertension, coronary artery disease, and insulin-dependent diabetes mellitus presents to the emergency department with a complaint of painful sores on the top of her left foot. Updated 2022 Dec 1]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Necrobiosis Lipoidica.
The ECG is just a test: a Bayesian approach to acute coronary occlusion If a patient with a recent femur fracture has sudden onset of pleuritic chest pain, shortness of breath, and hemoptysis, the D-dimer doesn’t matter: the patient’s pre-test likelihood for PE is so high that they need a CT. But does this matter?
1] But there are multiple other abnormalities that make this ECG diagnostic of Occlusion MI, localized likely to the right coronary artery: 1. Inferior hyperacute T waves, which have been added to the 2022 ACC consensus on chest pain as a “STEMI equivalent”[3] 3. J Am Coll Cardiol 2022 4. De Alencar Neto. Int J Cardiol 2024 2.
Upon further research in the 1970’s, retrospective data from autopsies of those patients showed coronary aneurysms 5 Pathophysiology: Kawasaki Disease is a vasculitis of medium sized arteries. Tomisaku Kawasaki, who noticed 50+ similar pediatric presentations between the years 1961 and 1967.
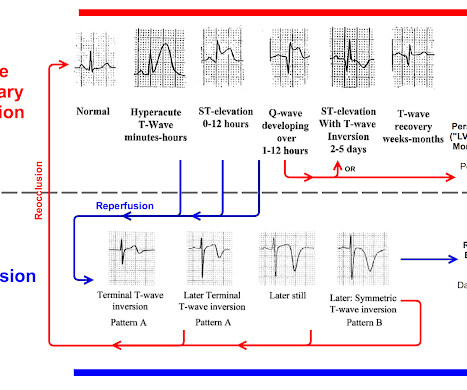
A comparison of electrocardiographic changes during reperfusion of acute myocardial infarction by thrombolysis or percutaneous transluminal coronary angioplasty. Total coronary occlusion, if very brief, may have minimal infarction and yet be very dangerous. Pattern A evolves into Pattern B. Am Heart J. 2000;139:430–436. Am J Cardiol.
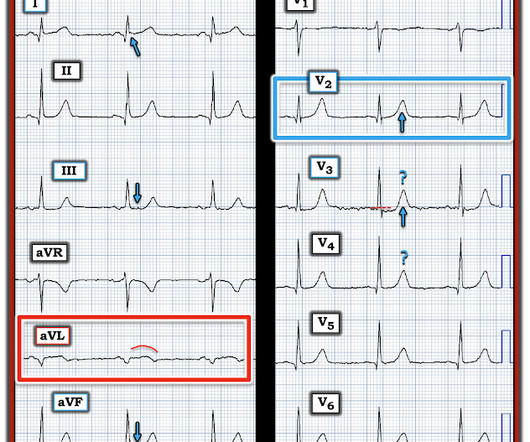
In the context of this woman in her 60s who has known coronary disease ( and who is now presenting with acute chest discomfort ) — I interpreted neighboring leads V1 and V2 as part of the same acute process suggested by the QRST in lead V3. For more on Precordial Swirl — See the October 15, 2022 post in Dr. Smith's ECG Blog ).
This new ECG was still interpreted as STEMI and the patient was taken to the cath lab where the angiogram showed completely normal coronary arteries throughout. Smith : this ECG is definitely not OMI, but could be mistaken for Swirl pattern, which is a septal OMI with STE in V1 and STD in V6. Unfortunately no echo was available.
NSTEMI dichotomy is not sensitive for true occlusion MI or acute coronary occlusion. “The application of STEMI ECG criteria on a standard 12-lead ECG alone will miss a significant miry of patients who have acute coronary occlusion.” NCSE is likely more common than we think.
The patient was treated as possible NSTEMI and underwent coronary angiography about 4 hours after presentation. TIMI 3 means the rate of passage of dye through the coronary artery is normal by angiography.) Initial hsTnI was 384 ng/L. The report describes a 60% proximal LAD lesion with TIMI 3 flow.
Past medical history includes coronary stenting 17 years prior. Cardiology was consulted and the patient underwent coronary angiogram which showed diffuse severe three-vessel disease. Coronary angiogram shows diffuse severe three-vessel disease. Initial ED ECG: What do you think? Why did I say that?
For the same reason, you should not delay coronary angiography because pain resolves with morphine. When I see this, I always look at V2 for any evidence of posterior OMI (STD, or loss or inversion of T-wave, or downsloping ST segment: there is a negative T-wave ), and V6 for any STE (normal). So I would be worried about inferior OMI.
Thanks in part to rapid bedside diagnosis, the patient was able to avoid emergent coronary angiography. Consider the following: We become attuned to looking for acute coronary occlusion in patients who present with acute symptoms to the ED ( E mergency D epartment ). What do you do clinically when the ECG looks like this?
Date: May 24th, 2022 Reference: Broder et al. Date: May 24th, 2022 Reference: Broder et al. AEM May 2022 Guest Skeptic: Dr. Justin Morgenstern is an emergency physician and the creator of the #FOAMed project called First10EM.com Case: A 33-year-old male presents to the emergency department (ED) complaining of abdominal pain.
Although predicting the "culprit" artery of acute coronary occlusion is often straightforward ( ie, based on the distribution of leads with ST elevation and leads with reciprocal ST depression ) — this is not always the case. The April 8, 2022 post by Drs. See Discussion in the June 29, 2024 post of Dr. Smith' ECG Blog ).
The coronary angiogram revealed no critical stenosis, or acute plaque ulceration. Takotsubo should be a diagnosis of exclusion after angiography reveals no obstructive coronary disease, and repeat Echo displays left ventricular recovery. A 12 Lead ECG was recorded secondary to bizarre telemetry findings at bedside.
2022 Jan;51:384-387. 2022 May;55:180-182. 2022 May;55:180-182. Epub 2022 Mar 17. I have here 38 cases of "Computer Normal" ECGs which were critically abnormal and the vast majority are missed acute coronary occlusions (Missed Acute OMI) and most were recognized by the physician. by being interrupted??? 2021.11.023.
The patient is an older woman with known coronary disease and an ICD-Pacemaker implanted because of a history of VT ( V entricular T achycardia ). However , this patient is having chest discomfort, and by definition then she should be considered not to be stable. Is this: 1. In either case, prompt cardioversion is indicated.
You can easily imagine this patient getting one of several diagnoses -- vasospasm, MINOCA , pericarditis, or maybe even no diagnosis at all beyond "non-obstructive coronary artery disease." Another option would be to use Optical Coherence Tomography for Coronary Imaging ). That plaque is at risk of thrombosing again.
Coronaries were clean. There ARE Signs of a Repolarization Variant: Among the many posts in which we've reviewed cases of repolarization variants — is the May 23, 2022 post. If a final test was perceived as "needed" — perhaps a normal coronary CT angiogram could have helped to avoid cardiac catheterization. Real or just fake?"
A CT Coronary angiogram was ordered. Here are the results: --Minimally obstructive coronary artery disease. --LAD Although a lesion is not visible anatomically on this CT scan, coronary catheter angiography could be considered based on Cardiology evaluation." A repeat troponin returned at 0.45 CAD-RADS category 1. --No
As per Dr. McLaren — today's patient was lucky in that the acute coronary occlusion spontaneously reperfused — and the patient remained pain-free. There’s clear T wave inversion in III/aVF, which is reciprocal to subtle ST elevation and hyperacute T waves in I/aVL (broad, symmetric, and larger than the entire QRS in aVL).
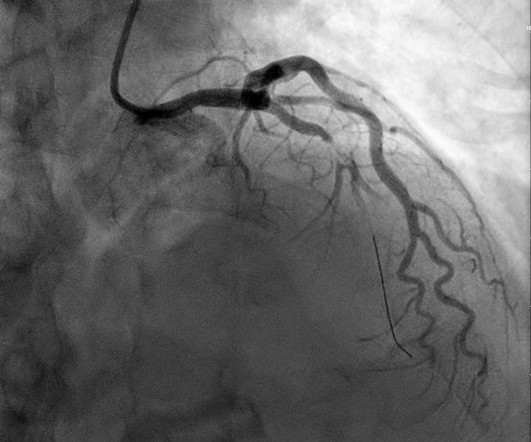
It shows a proximal LAD occlusion, in conjunction with a subtotally occluded LMCA ( Left Main Coronary Artery ). Upon contrast injection of the LMCA, the patient deteriorated, as the LMCA was severely diseased and flow to all coronary arteries ( LAD, LCx and RCA ) was compromised. He was taken immediately to the cath lab.
First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion. The new ACC expert consensus explains that: “STEMI ECG criteria on a standard 12-lead ECG alone will miss a significant minority of patients who have acute coronary occlusion. Take home 1.
6] Among 394 emergency department Code STEMI patients with acute culprit lesion requiring coronary interpretation, 16 (4.1%) presented with an ECG labeled ‘normal’ or ‘otherwise normal’ by computer interpretation. Written by Jesse McLaren Four patients presented with chest pain. minutes).
Comment by K EN G RAUER, MD ( 12/12 /2022 ): = I will summarize in 4 words the important message conveyed by Dr. Meyers in today's post = "Be Aware of Pseudo-Normalization!" In other words, to get from hyperacute T waves and STE to terminal T wave inversion, the ST and T wave must pass transiently through a state of near-normal.
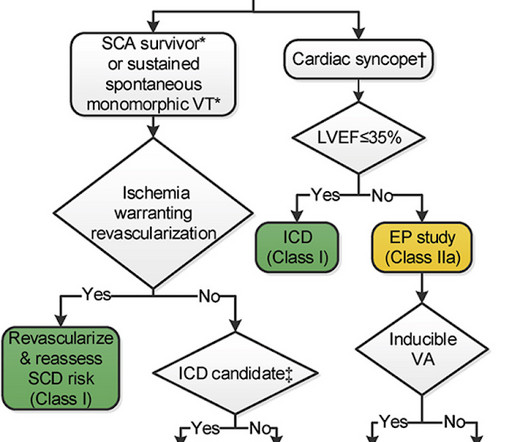
Other cardiac-related causes for syncope associated with acute MI may include malignant ventricular arrhythmias and bradyarrhythmias including AV block. The "good news" — is that a cardiac-related cause of syncope is unlikely if the initial ECG is normal, and cardiac monitoring in the ED fails to reveal significant arrhythmia.
American Gastroenterological Association issued a practice guideline in November 2022 recommending that semaglutide 2.4 GLP-1 agonists are also associated with improved ejection fraction, coronary blood flow, and cardiac output while reducing the risk of cardiovascular events, infarction size, and all-cause mortality. How do they work?
Autopsy shows coronary atherosclerosis and marked cardiomegaly with a thickened left ventricular wall. 3 : September 2022. An unknown EP reviews the report, determines that there is no reason to notify the patient, and documents nothing. Plaintiff : You told me you would call me if the radiology report was “different.” Tyler W et al.
The 50-something patient with history of coronary stenting and slightly reduced LV ejection fraction. which would suggest reduced rates of major adverse cardiac events with coronary artery bypass grafting." On the other hand, stable EKG over an hour in the setting of ongoing acute coronary syndrome is again unusual.
All coronary arteries were patent without atherosclerotic change. Dr. Myocarditis can be very difficult to separate from OMI on ECG, and often some form of coronary artery imaging will need to be done to rule out OMI. In any case, the ECG is diagnostic of severe ischemia and probably OMI. Concordant STE of 1 mm in just one lead or 2a.
And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! Association of intravenous morphine use and outcomes in acute coronary syndromes: Results from the CRUSADE Quality Improvement Initiative. Do NOT give it unless you are committed to the cath lab!! Cath attending is aware. Am Heart J.
Thus, this does NOT meet STEMI criteria (though, as of 2022, it is a formal "STEMI equivalent", assuming everyone agrees that this is de Winter morphology, for which there is currently no objective definition). Also, if you use the LAD OMI formula : QT = 420, RAV4 = 5 mm, QRSV2 = 6 mm, STE60V3 = 2.5 mm, the value is 22.2 (LAD What a farce.
Knowing the patient has a history of coronary disease could be relevant to today's case — as it should add to our suspicion of a new acute event. If this is the case — this size of a Qr wave in lead III, as well as the seemingly wide Q in lead aVF — would seem to suggest prior inferior infarction a t some point in the past.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content