This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Traditionally, emergency providers looked for signs of ST-segment elevation myocardial infarction (STEMI) to indicate the need for intervention. Emergency physicians have recognized for some time that there are many occlusions of the coronary arteries that do not present with classic STEMI criteria on the ECG.
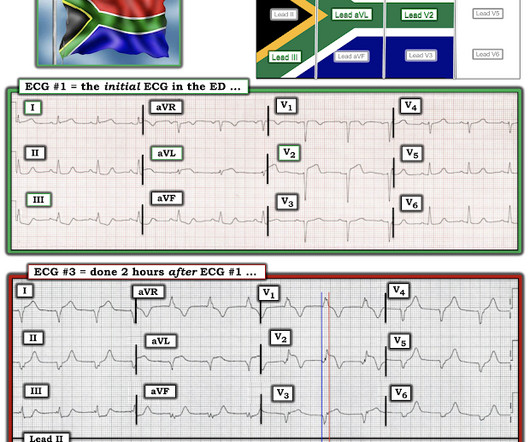
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. Compensatory enlargement was defined as being present when the total coronary arterial cross-sectional area at the stenotic site was greater than that at the proximal nonstenotic site. He was started on nitro gtt.
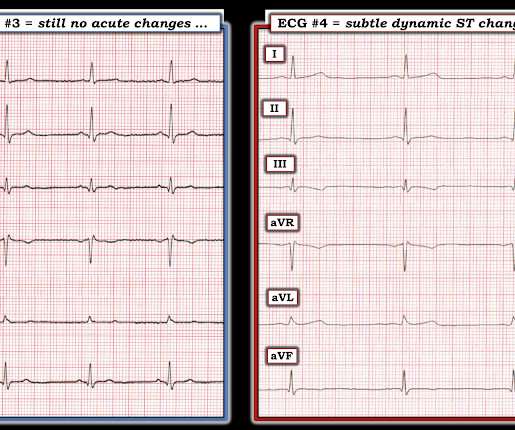
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Similarly, if a patient with known CAD presents with refractory ischemic chest pain, the ECG barely matters: the pre-test likelihood of acute coronary occlusion is so high that they need an emergent angiogram.
So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
Cath lab declined as it is not a STEMI." And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! Another myocardial wall is sacrificed at the altar of the STEMI/NonSTEMI mindset. Do NOT give it unless you are committed to the cath lab!! Cath attending is aware. Am Heart J.
Reference: emDOCs – NCSE Journal of Emergency Medicine – Review Case 4: 52-year-0ld male brought in by EMS with “code STEMI” ECG demonstrates ST depressions with rocket like T waves in V2-V4. This document covers high sensitivity troponin, risk disposition pathways, and STEMI equivalents. J Am Coll Cardiol.
But like many similar studies, the study was small (one year at one centre with no indication of the incidence of acute coronary occlusion), and it used as the gold standard the final cardiologist interpretation of the ECG - not the patient outcome! Despite serial ECGs being "STEMI negative", the cath lab was activated.
Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). A comparison of electrocardiographic changes during reperfusion of acute myocardial infarction by thrombolysis or percutaneous transluminal coronary angioplasty.
This certainly looks like an anterior STEMI (proximal LAD occlusion), with STE and hyperacute T-waves (HATW) in V2-V6 and I and aVL. How do you explain the anterior STEMI(+)OMI immediately after ROSC evolving into posterior OMI 30 minutes later? This caused a type 2 anterior STEMI. The April 8, 2022 post by Drs.
I sent this ECG to the Queen of Hearts (PMcardio OMI), and here is the verdict: You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form Then I learned that a Code STEMI was activated for concern of anterior "STEMI" in V1-V2. High sensitivity troponin I was 23 ng/L.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. Additionally, his cardiac telemetry monitor showed runs of accelerated idioventricular rhythm, a benign arrhythmia often associated with coronary reperfusion.
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." For the same reason, you should not delay coronary angiography because pain resolves with morphine. The case continues. Mukherjee, D.,
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
4,5] We have now formally studied this question: Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.[6] have published a number of warnings about the previous reassuring studies.[4,5]
The conventional machine algorithm interpreted this ECG as STEMI. See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI. Thanks in part to rapid bedside diagnosis, the patient was able to avoid emergent coronary angiography. When EMS found her, she was dyspneic and diaphoretic.
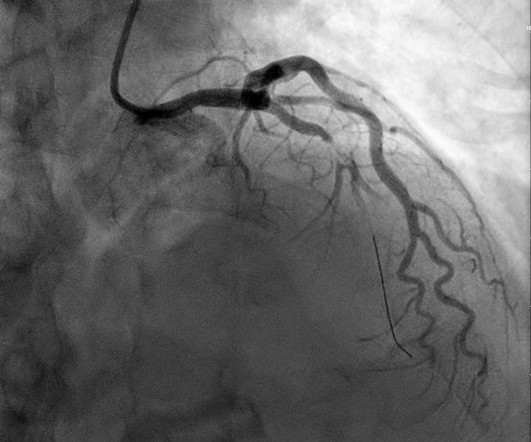
Smith , d and Muzaffer Değertekin a DIFOCCULT: DIagnostic accuracy oF electrocardiogram for acute coronary OCClUsion resuLTing in myocardial infarction. Coronary arteries cannot be assessed because the scan was not gated, but proximal segments of the coronary arteries seem to be open with some contrast. Again nothing diagnostic.
Subtle as a STEMI." (i.e., Here is the bottom line of the article: It is widely believed that hyperacute T-waves are a transitional state preceding ST Elevation 1–4 Thus, it is tempting to postulate that early cases of OMI will eventually evolve to STEMI; yet, our data contradicts that notion. This one is easy for the Queen.
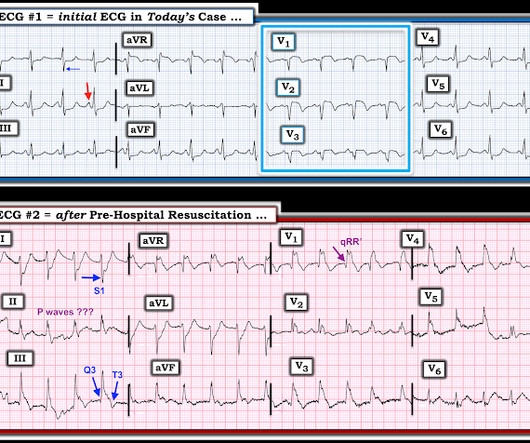
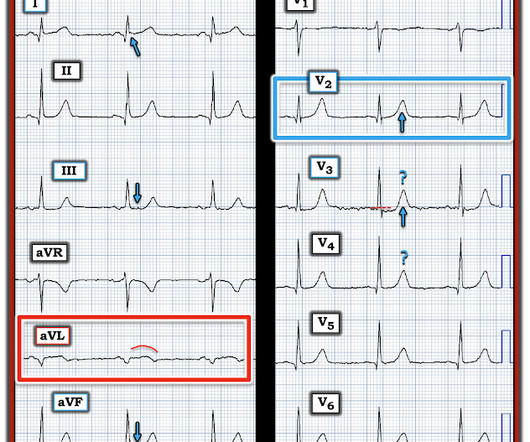
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. Figure-1: The initial ECG in today’s case.
A CT Coronary angiogram was ordered. Here are the results: --Minimally obstructive coronary artery disease. --LAD Although a lesion is not visible anatomically on this CT scan, coronary catheter angiography could be considered based on Cardiology evaluation." Transient STEMI is at high risk of re-occlusion.
Here they are: Patient 1, ECG1: Zoll computer algorithm stated: " STEMI , Anterior Infarct" Patient 2, ECG1: Zoll computer algorithm stated: "ST elevation, probably benign early repolarization." He diagnosed anterior "STEMI" and activated the cath lab. 25 minutes later, EMS called back with this new ECG: Super obvious STEMI(+) OMI.
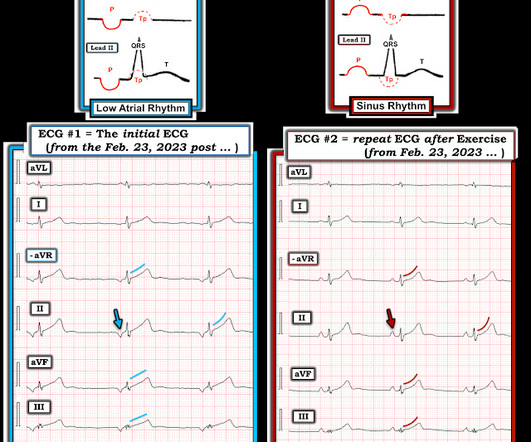
In the available view of the sinus rhythm, we see normal variant STE which probably meets STEMI criteria in V4 and V5. In other words, the inferior "ST elevation" is due to the abnormal rhythm, and does not signify OMI or STEMI in any way. The angiogram showed completely normal coronary arteries.
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. It shows a proximal LAD occlusion, in conjunction with a subtotally occluded LMCA ( Left Main Coronary Artery ). The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chest pain.
She was diagnosed with a Non-STEMI and kept overnight for a next day angiogram. She went to angio and had normal coronaries. Medics recorded the above ECG and called a STEMI alert. No d-dimer or CT pulmonary angiogram was done when they discovered that she had normal coronary arteries. Her troponin I returned at 900 ng/L.
There is an obvious inferior posterior STEMI(+) OMI. Methods Retrospective study of consecutive inferior STEMI , comparing ECGs of patients with, to those without, RVMI, as determined by angiographic coronary occlusion proximal to the RV marginal branch. What is the atrial activity? Is it sinus arrest with junctional escape?
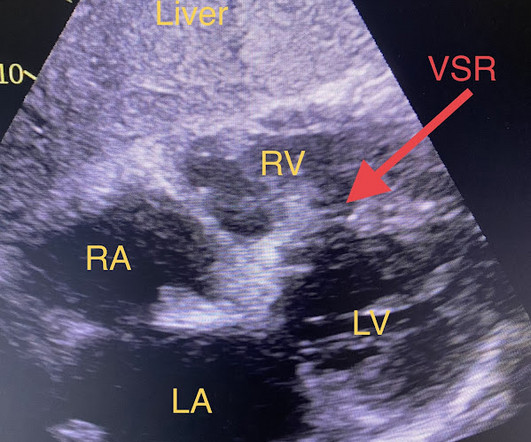
Another possible cause of pseudonormalization of T waves mentioned many times on this blog is the pseudonormalization caused by re-occlusion of an infarct related reperfused coronary artery. A mong patients with STEMI, ventricular septal rupture is the most common and free wall rupture is the least common.
"Unfortunately, the cardiologist waited until the next day to refer the patient for angiography and intervention because patient did not meet criteria for "STEMI"." The coronary angiography showed a 100% ostial main (obtuse) marginal occlusion!" Dominant right coronary, atherosclerotic and calcified. Peak troponin: 128,000 ng/L.
The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. The paramedic notes called STEMI into question: “EMS disagree with monitor for STEMI callout. Coronaries were normal, as was serial troponin. Vitals were normal.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? Incidence of an acute coronary occlusion.
Unfortunately you can see that the conventional Zoll algorithm sees nothing even to suggest AMI, let alone STEMI. For review on how I apply the Mirror Test I devised — See My Comment in the September 21, 2022 post in Dr. Smith's ECG Blog ). = Really unusual to me that QOH V1 only has low confidence, but at least its correct.
In the context of remote rural communities, this can help emergency physicians advocate for their patients, and reduce reperfusion delays by days for STEMI(-)OMI == MY Comment , by K EN G RAUER, MD ( 9/8 /2023 ): == Today’s case is distinguished by its occurrence in a remote rural community ( where the nearest cath lab is a plane ride away ).
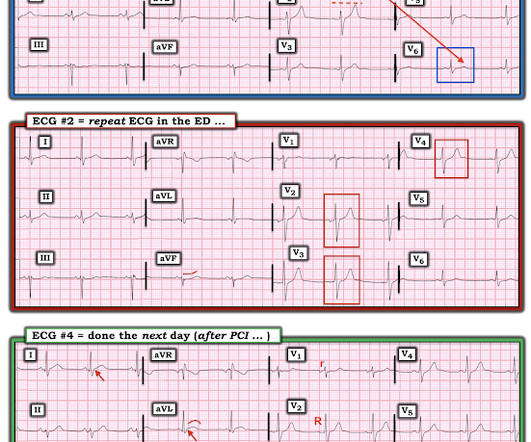
But because there was no new ST elevation, the ECG was signed off as “STEMI negative” and the patient waited to be seen. But the ECG still doesn’t meet STEMI criteria. It was therefore interpreted as “no STEMI” and the patient was treated with dual anti-platelets and referred to cardiology as “NSTEMI.” the cardiologist 5.
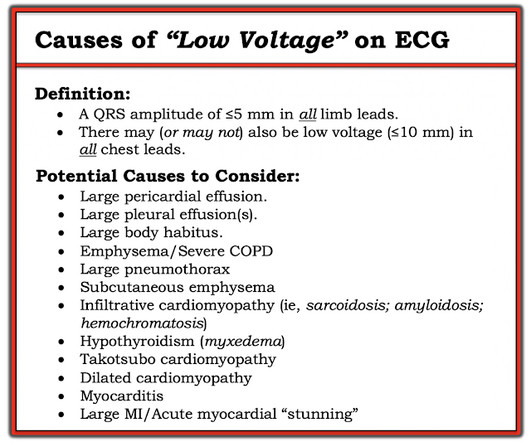
Hospital Course The patient was taken emergently to the cath lab which did not reveal any significant coronary artery disease, but she was noted to have reduced EF consistent with Takotsubo cardiomyopathy. Such cases are classified as MINOCA (Myocardial Infarction with Non-Obstructed Coronary Arteries). It can only be seen by IVUS.
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below). In a study last year, 14.4%
So we activated the Cath Lab Angiogram: Impression and Recommendations: Culprit for the patient's anterior ST segment myocardial infarction and out of hospital V-fib cardiac arrest is a thrombotic occlusion of the mid LAD The first troponin returned barely elevated at 36 ng/L (URL = 35) In our study of initial troponin in STEMI, 26.8%
The ED provider ordered a coronary CT scan to assess the patient for CAD. His EKG with worse pain now shows enough ST elevation to meet STEMI criteria. The EKG was read by the conventional computer algorithm as diagnostic of “ACUTE MI/STEMI”. The patient started receiving medications for “STEMI” (including heparin!!!)
It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers. All coronary arteries were patent without atherosclerotic change. . == Below is the ECG of Patient #2 — as interpreted by the QOH. The ECG is diagnostic of occlusion myocardial infarction (OMI).
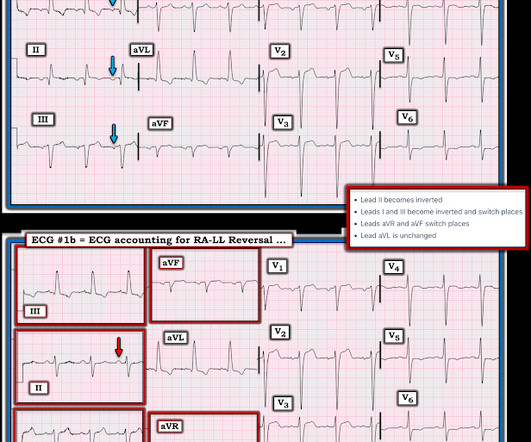
Here, I do not see OMI (although the ECG is falsely STEMI positive with just over 1 mm STE in V1 and about 2.5 Therefore the impulse must have originated somewhere lower in the atria, perhaps near the coronary sinus. The April 17, 2022 post ( Leads V1,V2 misplacement ). The May 5, 2022 post ( LA-RA reversal ).
Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. This was several months after the 2022 ACC Guidelines adding modified Sgarbossa criteria as a STEMI equivalent in ventricular paced rhythm). LAFB, atrial flutter, anterolateral STEMI(+) OMI. Limkakeng AT.
The ECG is diagnostic for acute transmural infarction of the anterior and lateral walls, with LAD OMI being the most likely cause (which has various potential etiologies for the actual cause of the acute coronary artery occlusion, the most common of which is of course type 1 ACS, plaque rupture with thrombotic occlusion). Aspirin 81 mg daily.
The ECG was read as "No STEMI" and the patient was treated like an average chest pain patient (despite the fact that a chest pain patient with active pain and active subendocardial ischemia is very high risk). The De Winter ECG pattern: morphology and accuracy for diagnosing acute coronary occlusion: systematic review. Eur J Emerg Med.
Knowing the patient has a history of coronary disease could be relevant to today's case — as it should add to our suspicion of a new acute event. If this is the case — this size of a Qr wave in lead III, as well as the seemingly wide Q in lead aVF — would seem to suggest prior inferior infarction a t some point in the past.
Moreover, the research which appears to confirm this idea was indeed in relation to the circumflex, but they did not study Occlusion ; rather, they studied asymptomatic coronary disease. I showed conclusively that this is a common finding in normal ECGs, though it is more common in LAD Occlusion than in norml variant STE.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content