This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
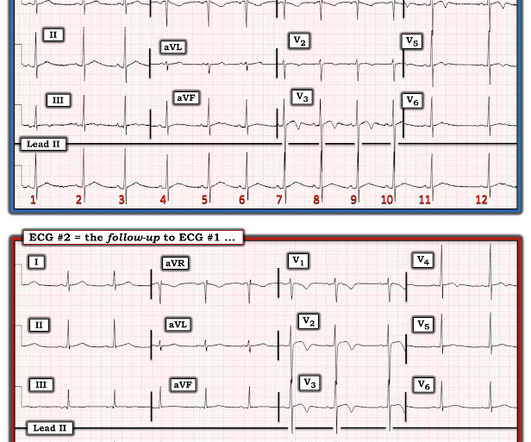
The conventional machine algorithm interpreted this ECG as STEMI. See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI. Here is lead I from ECGs 1 and 2 shown side-by-side to highlight the change in axis from borderline right to completely normal. Her ECG is shown below: What do you think?
Post cath ECG: Now there are hyperacute T-waves again, and recurrent ST depression in V2 This ECG would normally diagnostic of OMI until proven otherwise No further troponins were measured, but it looks like there is recurrent OMI Next day: A CT Coronary Angiogram was done (CTCA) CARDIAC MORPHOLOGY AND FUNCTION: 1. IMPRESSION: 1.
There is an obvious inferior posterior STEMI(+) OMI. We recorded an ECG in which V1-V3 were put in the position of V4R-V6R, and V4-6 were placed in V7-9 to (academically) confirm posterior OMI. 1 mg of Atropine was given and the heart rate increased transiently to 60. What is the atrial activity? How would one tell? What to do?
Two recent interventions have proven in randomized trials to improve neurologic survival in cardiac arrest: 1) the combination of the ResQPod and the ResQPump (suction device for compression-decompression CPR -- Lancet 2011 ) and 2) Dual Sequential defibrillation. Figure-1: The initial ECG in today's case — obtained after ROSC.
But these cases show the potential dangers of delayed recognition and treatment of inferior reperfusion Take away 1. Rather than using terms like “STEMI” and “Wellens”, it’s more helpful to describe the underlying pathology and ECG pattern pattern: Occlusion MI, and reperfusion T wave inversion 4. JAMA Intern Med 2019 9.
As always, LAD OMI need not meet STEMI criteria and usually does NOT! Here are many examples which we have already posted: 5 of LVH mimicking Precordial Swirl 1 case (Case 6) of LVH mimicking precordial swirl, but it is actually LVH + posterior OMI 14 Cases (Cases 7-20) of OMI with Precordial Swirl First, 5 mimics: Case 1.
mm of ST segment elevation, V2 and V3 have 1 mm of elevation, v4 has 2 mm of elevation and v5 around 1.5 Note 1: Levels were significantly lower in takotsubo that presented with T-wave inversion. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al. Learning Points: 1. What do you think? V1 has 0.5
Anterior STEMI? Young African American Male with Atypical Stabbing Chest Pain Benign T-wave Inversion: view video or read text == Comment by K EN G RAUER, MD ( 5/19/2022 ): == Concise but important presentation by Dr. Meyers that emphasizes the following points: The History is KEY. Activate the Cath Lab?
Easy LINK — [link] — My New E CG P odcasts ( 5/28/2024 ): These podcasts are part of the Mayo Clinic Cardiovascular CME Podcasts Series ( "Making Waves" ) — hosted by Dr. Anthony Kashou. 2:25 — Dr. Grauer: The 1st Error : Too many clinicians in 2024 are still stuck in the outdated millimeter-based STEMI Paradigm”.
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." Case continued She was loaded with aspirin 325 mg, and repeat troponin drawn around the time of EKG 1 resulted at 267 ng/L. At midnight.
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. Patients that develop a Type 1 pattern without any precipitating or provoking factors have a risk of SCD of 0.5-0.8% per year incidence of SCD in this cohort [1].
If you were thinking that this is not anterior OMI because there is no reciprocal ST depression , it is important to remember that half of anterior STEMI do NOT have any reciprocal ST depression. There are some unusual ECG findings in today's tracing ( that I labeled in Figure-1 ). Anterior OMI? Pericarditis?
Despite the clinical context, Cardiology was consulted due to concerns for a "STEMI". Hyperkalemia mimics STEMI and OMI in many distributions, but probably the most common is the Brugada morphology in V1-V2 which mimics anterior OMI for those who cannot recognize the Brugada pattern. Limb lead reversal can be easily recognized.
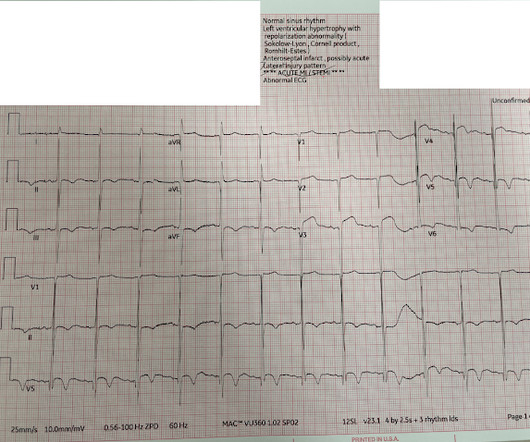
Even before we have clinical context, this ECG simply does not appear concerning for OMI, notwithstanding the machine's interpretation ** ** ACUTE MI / STEMI ** **. But in the world of STEMI, this is a challenging ECG to most. Pendell Meyers , Aaron E. I suspect most blog readers did not struggle with this one. Baker , Shifa R.
The status of the patients chest pain at this time is unknown : EKG 1, 1300: There is sinus tachycardia and artifact of low and high frequency. Supply-demand mismatch can cause ST Elevation (Type 2 STEMI). Also see these posts of Type II STEMI. Also see these posts of Type II STEMI. An EKG was immediately recorded.
When I saw this (presented at a conference), I immediately thought it looked like Thype 1 Brugada phenocopy (in other words, Type 1 Brugada ECG pattern ). If the QRS is prolonged, then the differential includes: 1. Criteria for Type 1 Morphology: 1. A flat ST segment will have a Corrado index greater than 1.
1:45, case start To orient you to this screen, the top is obviously ECG waveforms. 1:51, diagnostic RCA angiography At this point, the patient very clearly has a diagnosis of OMI, especially since we visualized embolism within the PDA. & Falk, E. Papadopoulou, E., link] Falk, E., Bossone, E., Tang, Z.,
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content