This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. Here is his most recent previous ECG: This was recorded after intervention for inferior STEMI (with massive ST Elevation, see below), and shows inferior Q-waves with T-wave inversion typical of completed inferior OMI. ng/mL (quite large).
He arrived to the ED with severe hypotension, heart rate in the 70s, unable to follow commands but moving all extremities requiring restraint and sedation, respiratory rate around 24/min being supported with bag valve mask, with significant hypoxemia. Meyers and Smith in the October 15, 2022 post of Dr. Smith's ECG Blog ).
So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
With a new protocol and Pulsara, Metropolitan Emergency Medical Services can now transport eligible pediatric behavioral health patients directly to behavioral health facilities—resulting in a 44% decrease of pediatric behavioral health patients transported to the ED. Download the case study or read on to learn more!
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. He arrived to the ED by helicopter at 1507, about three hours after the start of his chest pain while chopping wood around noon. He wrote most of it and I (Smith) edited.
The interventional cardiologist then canceled the activation and returned the patient to the ED without doing an angiogram ("Not a STEMI"). Despite the ACC guidelines for posterior STEMI, the cardiologist again refused to take the patient to the cath lab. mm STE in the posterior leads.
On ED arrival GCS is 3, there are rapid eye movements to the right but no other apparent seizure activity. Official diagnosis requires EEG, which is not something we can typically obtain in the ED. This document covers high sensitivity troponin, risk disposition pathways, and STEMI equivalents.
Our data corroborate that immediate management of a patient with a normal automated triage ECG reading is not modified by real-time ED physician ECG interpretation." Smith comment: we showed that the first troponin, even in full-blown STEMI, is negative 25% of the time. But according to Langlois-Carbonneau et al.,
4,5] We have now formally studied this question: Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.[6] have published a number of warnings about the previous reassuring studies.[4,5]
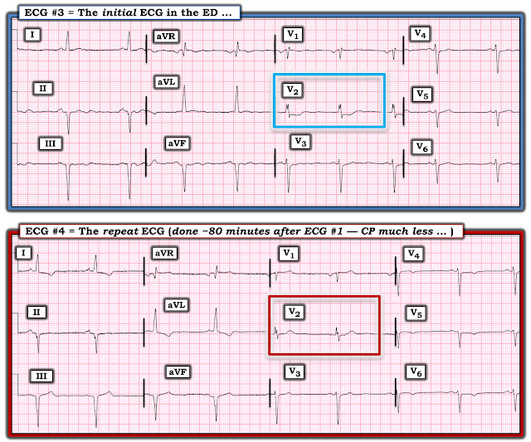
It was present on arrival at triage but then resolved before bed placement in the ED. Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). It is a ssociated with mild dyspnea on exertion. Aspirin given.
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
Unknown algorithm The Queen gets it right Case 4 How unreliable are computer algorithms in the Diagnosis of STEMI? The patient's prehospital ECG showed that there was massive STEMI and these are hyperacute T-waves "on the way down" as they normalize. The Queen gets it right First ED ECG: Hyperacute T-waves persist.
Both cases had an EMS ECG that was transmitted to the ED physician asking "should we activate the cath lab?" Here they are: Patient 1, ECG1: Zoll computer algorithm stated: " STEMI , Anterior Infarct" Patient 2, ECG1: Zoll computer algorithm stated: "ST elevation, probably benign early repolarization." What do you think?
Written by Jesse McLaren A 75 year-old patient with diabetes and end stage renal disease was sent to the ED after dialysis for three days of nausea, vomiting, loose stool, lightheadedness and fatigue. They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. RR18 sat 99% HR 90 BP 90/60, afebrile.
Subtle as a STEMI." (i.e., Here is the bottom line of the article: It is widely believed that hyperacute T-waves are a transitional state preceding ST Elevation 1–4 Thus, it is tempting to postulate that early cases of OMI will eventually evolve to STEMI; yet, our data contradicts that notion. This one is easy for the Queen.
This certainly looks like an anterior STEMI (proximal LAD occlusion), with STE and hyperacute T-waves (HATW) in V2-V6 and I and aVL. On arrival to the ED, this ECG was recorded: What do you think? How do you explain the anterior STEMI(+)OMI immediately after ROSC evolving into posterior OMI 30 minutes later?
Sent by anonymous, written by Pendell Meyers, reviewed by Smith and Grauer A man in his 40s presented to the ED with HTN, DM, and smoking history for evaluation of acute chest pain. In the available view of the sinus rhythm, we see normal variant STE which probably meets STEMI criteria in V4 and V5. Triage ECG: What do you think?
[link] Case continued She arrived in the ED and here is the first ED ECG. STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. I don't know if her pain was getting better or not. From Gue at al.
Written by Jesse McLaren Two patients in their 70s presented to the ED with chest pain and RBBB. The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. Do either, both, or neither have occlusion MI? Vitals were normal.
The neighbor recorded a systolic blood pressure again above 200 mm Hg and advised her to come to the ED to address her symptoms. Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI."
The conventional machine algorithm interpreted this ECG as STEMI. See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI. Consider the following: We become attuned to looking for acute coronary occlusion in patients who present with acute symptoms to the ED ( E mergency D epartment ).
Here is his ED ECG: There is bradycardia with a junctional escape. There is an obvious inferior posterior STEMI(+) OMI. Methods Retrospective study of consecutive inferior STEMI , comparing ECGs of patients with, to those without, RVMI, as determined by angiographic coronary occlusion proximal to the RV marginal branch.
male presents to the ED at 6:45 AM with left sided chest dull pressure that woke him up from sleep at 3am. He arrived to the ED at around 6:45am, and stated the pain has persisted. Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. The pain radiated to both shoulders.
Case An 82 year old man with a history of hypertension presented to the ED with chest pain at 1211. The ED provider ordered a coronary CT scan to assess the patient for CAD. His pain suddenly became much worse in the ED and he became acutely diaphoretic, dizzy, and hypotensive. There is pericardial tamponade.
Prior episodes had simply resolved after brief symptoms, but the current episode had lasted for 2 hours without improvement, so she presented to the ED. At triage she stated her pain is still persistent, but it is mildly improved compared to when she decided to come to the ED. No diaphoresis or vomiting. How to Check Your Findings.
In the context of remote rural communities, this can help emergency physicians advocate for their patients, and reduce reperfusion delays by days for STEMI(-)OMI == MY Comment , by K EN G RAUER, MD ( 9/8 /2023 ): == Today’s case is distinguished by its occurrence in a remote rural community ( where the nearest cath lab is a plane ride away ).
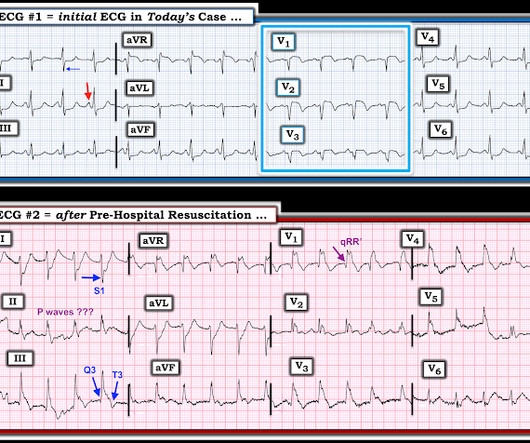
A 40-something with persistent Ventricular Fibrillation presented after attempted prehospital resuscitation A 40-something with no previous cardiac history presented to the ED in persistent Ventricular Fibrillation after attempted prehospital resuscitation. First — Some thoughts on the post -resuscitation ECG.
But because there was no new ST elevation, the ECG was signed off as “STEMI negative” and the patient waited to be seen. But the ECG still doesn’t meet STEMI criteria. It was therefore interpreted as “no STEMI” and the patient was treated with dual anti-platelets and referred to cardiology as “NSTEMI.” the cardiologist 5.
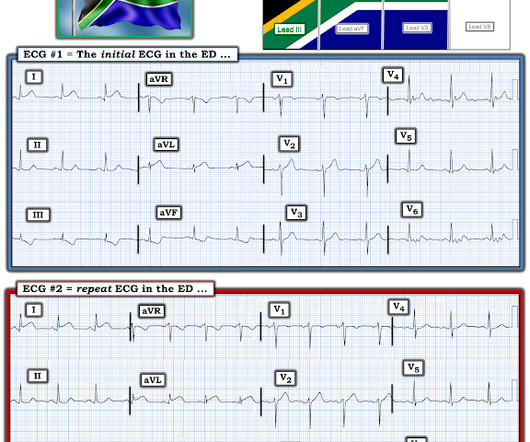
She was diagnosed with a Non-STEMI and kept overnight for a next day angiogram. Medics recorded the above ECG and called a STEMI alert. Her symptoms at the time ECG #1 was obtained were CP and SOB — yet interpretation of this initial tracing prompted a STEMI alert. Her troponin I returned at 900 ng/L.
He reported typical chest pain since 4H AM and arrived at our ED at 10h with ongoing chest pain. Unfortunately, the cardiologist waited until the next day to refer the patient for angiography and intervention because patient did not meet criteria for "STEMI"." The first ECG (10h14) showed TWI in inferior leads."
Since then, I started looking for OMI EKG findings and not just STEMI. Case "Male, 43yo, come to ED with Epigastric Pain started 3 hours ago. Remember: these findings above are included as STEMI equivalent findings in the 2022 ACC Expert Consensus Decision Pathway on ACS Patients in the ED. Vitals Signs: Normal."
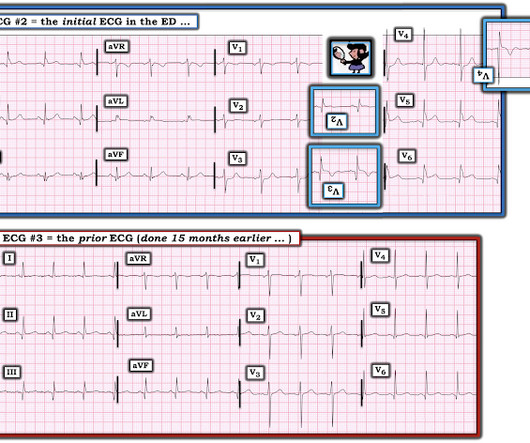
FIGURE 1: First ED EKG. FIGURE 2: Baseline ED from 2 months prior. FIGURE 3: Second ED EKG. Considering hyperacute T-waves have been accepted as STEMI equivalents, it is possible that pseudonormalization could gain more recognition as an indicator of ACS. 2022 Nov, 80 (20) 1925–1960. Click to enlarge.)
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below).
Edits by Meyers and Smith A man in his 70s with PMH of hypertension, hyperlipidemia, type 2 diabetes, CVA, dual-chamber Medtronic pacemaker, presented to the ED for evaluation of acute chest pain. Code STEMI was activated by the ED physician based on the diagnostic ECG for LAD OMI in ventricular paced rhythm. Limkakeng AT.
Later, I found old ECGs: 5 month prior in clinic: V5 and V6 look like OMI 9 months prior in clinic with no chest symptoms: V5 and V6 look like OMI 1 year prior in the ED with chest pain: V5 and V6 sure look like a STEMI For this ECG and chest pain in the ED, the Cath lab activated. But the angiogram was clean. There was no OMI.
His symptoms were reportedly resolved upon arrival to the ED. ED ECGs: 0814 0830 These show continued reperfusion with no evidence of reocclusion. I am going to code this as an acute STEMI as he had transient ST elevation which started to evolve in the emergency department but I think this is most appropriately termed STEMI."
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
A 40-something woman with diabetes and peripheral vascular disease who frequently needs the ED for chronic pain called 911 for sudden severe chest pain. Because of this, it was very difficult to record an ED ECG, but eventually it became possible: What do you think? The patient was very agitated and could not hold still.
An ECG was performed in the ED at 1554: Original image unavailable, this is the only recorded scanned ECG available. A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. He denied chest pain or shortness of breath.
There is clearly sufficient STE for STEMI criteria in leads V2 and aVL, but lead I has less than 1.0 mm of STE - thus, technically this ECG does not meet STEMI criteria, although it is a quite obvious OMI. This ECG was immediatel y discussed with the on-call cardiologist who said the ECG was "concerning but not a STEMI."
This is guideline approved by both ACC/AHA and by European guidelines. == Comment by K EN G RAUER, MD ( 6/1/2022 ): == I found serial evaluation of sequential tracings in today's case to be subtle — yet highly insightful. A patient with active chest pain and an otherwise unexplained elevated troponin should go to the cath lab.
One case sent by Dr. Sean Rees MD, written by Pendell Meyers, other case by Sam Ghali and Steve Smith Take a look at these two ECGs below from two patients in the ED, first without any clinical context. Physician interpretation: "No STEMI." Physician: "No STEMI." Full case details and outcomes are below.
Study idea: We should look at all OMIs who had a chest CT and compare to all patients with Non-OMI pathology who had a contrast chest CT and have radiologists blindly interpret the perfusion of the myocardium The cardiology fellow came down to the ED and said: "What are you worried about? This ST depression?" 2022.08.750 Section 5.2.2,
Of course, the bill for any episode of emergency department (ED) care can be substantial, exceeding the billed charges for equivalent care provided in some primary care offices. Now, many acute pyelonephritis patients receive an IV antibiotic, analgesia, and an antiemetic in the ED. This process required at least a full day.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content