This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Traditionally, emergency providers looked for signs of ST-segment elevation myocardial infarction (STEMI) to indicate the need for intervention. Emergency physicians have recognized for some time that there are many occlusions of the coronary arteries that do not present with classic STEMI criteria on the ECG.
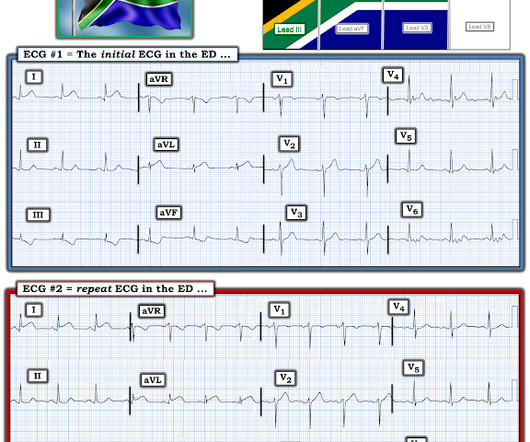
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
In 2020, MEMS adopted Pulsara to improve communication with area hospitals for time-sensitive emergencies such as stroke, STEMI, and trauma. Between 2022 and 2023, mental health calls accounted for 10% of MEMS’ overall call volume, with a noticeable surge in pediatric mental health cases.
If you were working in a busy emergencydepartment, would you like to be interrupted to interpret these ECGs or can these patients safely wait to be seen because of the normal computer interpretation? have published a number of warnings about the previous reassuring studies.[4,5]
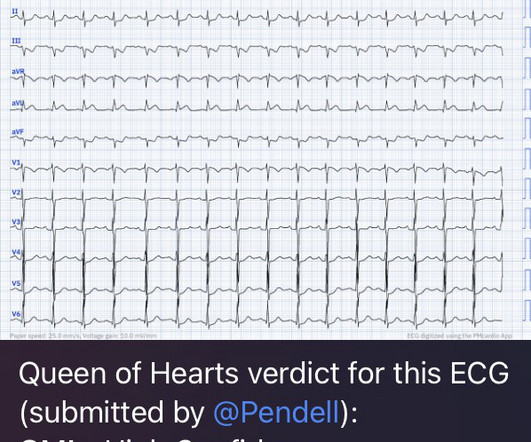
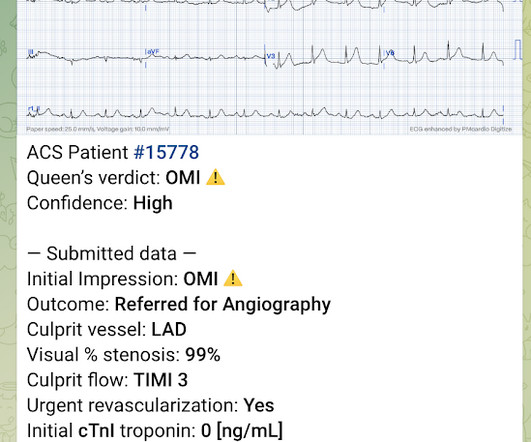
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergencydepartment with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion.
Reference: emDOCs – NCSE Journal of Emergency Medicine – Review Case 4: 52-year-0ld male brought in by EMS with “code STEMI” ECG demonstrates ST depressions with rocket like T waves in V2-V4. This document covers high sensitivity troponin, risk disposition pathways, and STEMI equivalents.
If we took this as the gold standard, we would conclude that the computer interpretation was safe and accurate at least accurate enough to not miss STEMI, and that physicians should not be interrupted to interpret it, because there would be no change in patient management. What is the gold standard for ECG interpretation: patient outcome!!!
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
Upon arrival to the emergencydepartment, a senior emergency physician looked at the ECG and said "Nothing too exciting." STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. From Gue at al.
A 50 year old presented to the emergencydepartment of a remote rural community (where the nearest cath lab is a plane ride away) with one hour of mild chest pain radiating to the back and jaw, and an ECG labeled ‘normal’ by the computer interpretation.
QOH versions 1 and 2 both say Not OMI, with high confidence, without any clinical context, despite the abnormal STE meeting STEMI criteria. Context: a man in his 40s presented to the emergencydepartment with 1 day of sudden onset chest pain. I sent this to our group without information and Dr. Smith responded: "Not OMI.
A 35-year-old male presented to the emergencydepartment complaining of chest pain that started 1.5 5 Studies looking at this phenomenon in the emergencydepartment setting for patients presenting with chest pain are lacking. Dr. Young is an emergency physician at Saint Francis Hospital and Medical Center, Hartford, Conn.
It was ongoing on arrival in the emergencydepartment. But because there was no new ST elevation, the ECG was signed off as “STEMI negative” and the patient waited to be seen. The emergency physician was called to see the patient 90 minutes later after the troponin I returned at 1100 ng/L. What do you think? Take home 1.
I finished my residency of Emergency Medicine and I’m working at a great EmergencyDepartment here in Brazil. Since then, I started looking for OMI EKG findings and not just STEMI. mm in lead I, thus not STEMI criteria) and was finally understood by the cardiologist.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
The remainder of his EmergencyDepartment stay was uneventful. The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chest pain)? Physician interpretation: "No STEMI." Physician: "No STEMI." He had no symptoms of ACS.
I am going to code this as an acute STEMI as he had transient ST elevation which started to evolve in the emergencydepartment but I think this is most appropriately termed STEMI." When is it anterior STEMI? Next day ECG: 2 Very instructive posts on LVH and OMI and Pseudo-OMI 1. Is this Acute Ischemia?
Emergency physicians have earned the right to “re-brand” ourselves as indispensable, money-saving change agents in the health care enterprise. Of course, the bill for any episode of emergencydepartment (ED) care can be substantial, exceeding the billed charges for equivalent care provided in some primary care offices.
Not seeing any changes on the initial 12 lead ECG, the emergency physician got a 15 lead ECG (below, where V4-6 are actually V4R and V7-8): There’s no posterior ST elevation but the anterior ST depression has resolved between the first and second ECG. Smith : this proves my impression that the inferior T-waves on the first ECG are hyperacute.
Emergent cardiac outcomes in patients with normal electrocardiograms in the emergencydepartment. Am J Emerg Med. 2022 Jan;51:384-387. These include about 60 occlusion MI (OMI) with clear ST segment elevation (none of which would be called “Normal” by the computer) and about 165 Non-STEMI. 2021.11.023.
Here is the repeat ECG at 52 minutes after arrival to triage: Obvious posterolateral STEMI Angiographic findings: 1. 2022 ACC expert consensus decision pathway on the evaluation and disposition of acute chest pain in the emergencydepartment: A report of the American college of cardiology solution set oversight committee. •
The HEART and EDACS scores are helpful to risk stratify patients with chest pain, but they hinge on accurate ECG interpretation: a low score doesn’t apply if the ECG shows STEMI(+)OMI, and shouldn’t be used for STEMI(-)OMI or OMI reperfusion either 2. Am J Emerg Med 2020 3. American Journal of Emergency Medicine 2022 4.
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergencydepartment with substernal chest pain for 3 hours prior to arrival. The screening physician ordered an EKG and noted his ashen appearance and moderate distress. Triage EKG: What do you think?
The limb leads have been removed because there was no ST elevation in those leads, the QRS complexes have been obscured because this is irrelevant to STEMI criteria, and red lines have been added to measure ST segment elevation. But STEMI criteria ignore all this and look at ST segments in isolation.
STEMI negative : the EMS automated interpretation read, “STEMI negative. According to the STEMI paradigm, the patient doesn’t have an acute coronary occlusion and doesn't need emergent reperfusion, so the paramedics can bring them to the ED for assessment, without involving cardiologists. Sinus bradycardia.”
There is worrisome T-wave inversion in inferior leads as well, which is another clue to LAD Occlusion In fact, this ECG meets STEMI criteria!! Why does the conventional algorithm not diagnose STEMI? Transient STEMI, serial ECGs prehospital to hospital, all troponins negative (less than 0.04 All intervals and the axis are normal.
A 69 year old woman with a history of hypertension presented to the emergencydepartment by EMS for evaluation of chest pain and shortness of breath. Supply-demand mismatch can cause ST Elevation (Type 2 STEMI). Also see these posts of Type II STEMI. Truly, the Marquette 12 SL algorithm correctly identifies this STEMI.
A 62 year old man with hyperlipidemia presented to a rural emergencydepartment with 7 hours of 3/10 chest pain. At 1210, the case was discussed with a cardiologist at a PCI capable facility, who accepted the patient for transfer, noting the ST depression in anterior leads as consistent with ischemia but not a STEMI.
He presented to the emergencydepartment for evaluation. 50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). Lets us consider two different clinical presentations. See Raitt et al.:
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




























Let's personalize your content