This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Traditionally, emergency providers looked for signs of ST-segment elevation myocardial infarction (STEMI) to indicate the need for intervention. Emergency physicians have recognized for some time that there are many occlusions of the coronary arteries that do not present with classic STEMI criteria on the ECG.
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. Here is his most recent previous ECG: This was recorded after intervention for inferior STEMI (with massive ST Elevation, see below), and shows inferior Q-waves with T-wave inversion typical of completed inferior OMI. ng/mL (quite large).
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. This was sent to me by an undergraduate name Hans Helseth, who is an EKG tech, but who is an expert OMI ECG reader. He wrote most of it and I (Smith) edited.
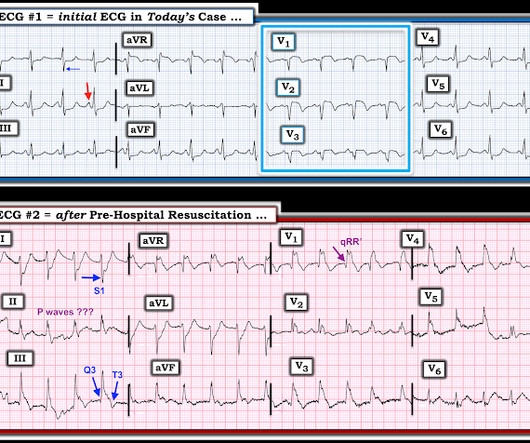
Despite anticipation by many that the initial post-resuscitation ECG will show an obvious acute infarction — this expected "STEMI picture" is often not seen. Meyers and Smith in the October 15, 2022 post of Dr. Smith's ECG Blog ). 15, 2022 post). Indeed, careful attention to detail is needed to appreciate the important findings.
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
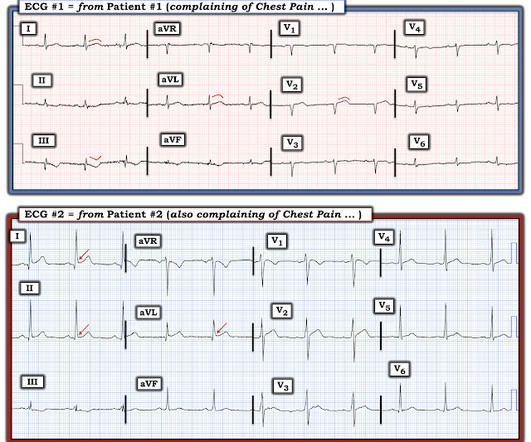
Here they are: Patient 1, ECG1: Zoll computer algorithm stated: " STEMI , Anterior Infarct" Patient 2, ECG1: Zoll computer algorithm stated: "ST elevation, probably benign early repolarization." He diagnosed anterior "STEMI" and activated the cath lab. 25 minutes later, EMS called back with this new ECG: Super obvious STEMI(+) OMI.
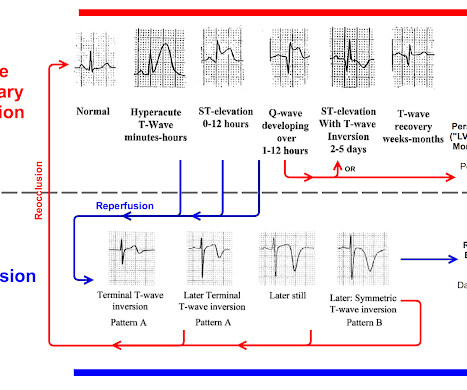
Subtle as a STEMI." (i.e., Here is the bottom line of the article: It is widely believed that hyperacute T-waves are a transitional state preceding ST Elevation 1–4 Thus, it is tempting to postulate that early cases of OMI will eventually evolve to STEMI; yet, our data contradicts that notion. This one is easy for the Queen.
Cath lab declined as it is not a STEMI." And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! Another myocardial wall is sacrificed at the altar of the STEMI/NonSTEMI mindset. Do NOT give it unless you are committed to the cath lab!! Cath attending is aware. Abstract 556.
So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
If we took this as the gold standard, we would conclude that the computer interpretation was safe and accurate at least accurate enough to not miss STEMI, and that physicians should not be interrupted to interpret it, because there would be no change in patient management. What is the gold standard for ECG interpretation: patient outcome!!!
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. Review of the 2 ECGs in today's case is insightful ( Figure-1 ): The initial ECG shows sinus rhythm, LAHB and meets Peguero Criteria for LVH ( See My Comment in the August 15, 2022 post of Dr. Smith's ECG Blog for more on LVH criteria ).
Reference: emDOCs – NCSE Journal of Emergency Medicine – Review Case 4: 52-year-0ld male brought in by EMS with “code STEMI” ECG demonstrates ST depressions with rocket like T waves in V2-V4. This document covers high sensitivity troponin, risk disposition pathways, and STEMI equivalents.
4,5] We have now formally studied this question: Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.[6] Written by Jesse McLaren Four patients presented with chest pain. have published a number of warnings about the previous reassuring studies.[4,5]
In 2020, MEMS adopted Pulsara to improve communication with area hospitals for time-sensitive emergencies such as stroke, STEMI, and trauma. Between 2022 and 2023, mental health calls accounted for 10% of MEMS’ overall call volume, with a noticeable surge in pediatric mental health cases.
Unknown algorithm The Queen gets it right Case 4 How unreliable are computer algorithms in the Diagnosis of STEMI? The patient's prehospital ECG showed that there was massive STEMI and these are hyperacute T-waves "on the way down" as they normalize. It is not yet available, but this is your way to get on the list. 2 cases at once!
Its hard to measure the STE in I exactly with the moving baseline, but there is almost certainly not enough STE to meet STEMI criteria. The ACC recognizes these findings as formal STEMI equivalents (though they do not define how to find them). They are symmetric, fat, convex on both sides, etc.
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. Potassium was normal. This is not unusual.
Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). As far as I can tell, there is only one randomized trial of immediate vs. delayed intervention for transient STEMI. Labs ordered but not yet drawn.
This certainly looks like an anterior STEMI (proximal LAD occlusion), with STE and hyperacute T-waves (HATW) in V2-V6 and I and aVL. How do you explain the anterior STEMI(+)OMI immediately after ROSC evolving into posterior OMI 30 minutes later? This caused a type 2 anterior STEMI.
September 2022 Guest Skeptic: Dr. Justin Morgenstern is an emergency physician and the creator of the #FOAMed project called www.First10EM.com Case: You are working an overnight shift at a small rural hospital. A post-arrest ECG doesn’t show any signs of STEMI. Date: February 1, 2023 Reference: Wolfrum et al. Circulation. Circulation.
This was a machine read STEMI positive OMI. The meaning of this quote is that at times, something as obvious as the dramatic anterior lead ST elevation that we see in today's tracing is not the result of an acute LAD STEMI. His ECG is shown below. Pretty obvious anterior current of injury. What would you guess is the culprit artery?
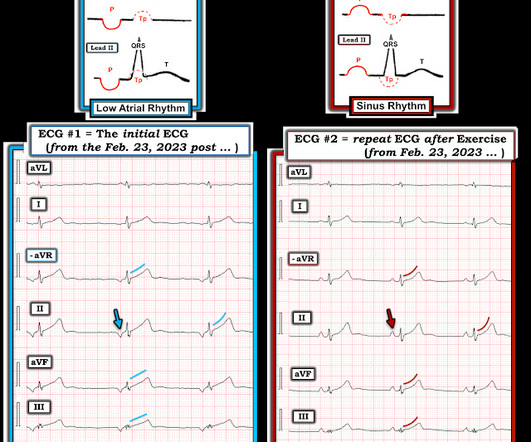
In the available view of the sinus rhythm, we see normal variant STE which probably meets STEMI criteria in V4 and V5. In other words, the inferior "ST elevation" is due to the abnormal rhythm, and does not signify OMI or STEMI in any way. This situation has been named "Emery phenomenon." YOU TOO CAN HAVE THE PM Cardio AI BOT!!
As always, LAD OMI need not meet STEMI criteria and usually does NOT! Septal STEMI with ST elevation in V1 and V4R, and reciprocal ST depression in V5, V6 Case 8. Missed LAD Occlusion with Swirl, peak trop 80 ng/mL (equivalent to 80,000 ng/L), diagnosed as "Non-STEMI" Case 9. A 49 year old man with chest pain.
In the context of remote rural communities, this can help emergency physicians advocate for their patients, and reduce reperfusion delays by days for STEMI(-)OMI == MY Comment , by K EN G RAUER, MD ( 9/8 /2023 ): == Today’s case is distinguished by its occurrence in a remote rural community ( where the nearest cath lab is a plane ride away ).
It has been estimated that in the aggregate, they occur at a rate of about 3 per 1000 patients with acute MI, and most of these events occur in patients with STEMI. It has been estimated that in the aggregate, they occur at a rate of about 3 per 1000 patients with acute MI, and most of these events occur in patients with STEMI.
STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. This has resulted in an under-representation of STEMI MINOCA patients in the literature. I don't know if her pain was getting better or not.
There is an obvious inferior posterior STEMI(+) OMI. Methods Retrospective study of consecutive inferior STEMI , comparing ECGs of patients with, to those without, RVMI, as determined by angiographic coronary occlusion proximal to the RV marginal branch. What is the atrial activity? Is it sinus arrest with junctional escape?
The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chest pain)? Physician interpretation: "No STEMI." Physician: "No STEMI." Cardiologist interpretation: "Technically does not meet STEMI criteria but concerning for ischemia."
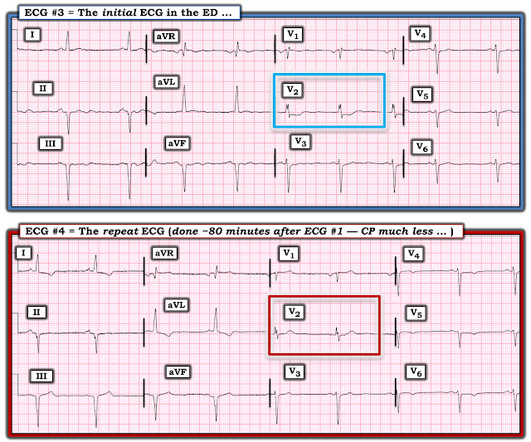
Comment by K EN G RAUER, MD ( 12/12 /2022 ): = I will summarize in 4 words the important message conveyed by Dr. Meyers in today's post = "Be Aware of Pseudo-Normalization!" Failure to do so may result in overlooking subtle ST-T wave changes in a patient "in passage" from a frank STEMI toward reperfusion changes.
This is documented as a STEMI in the clinical notes and in the cath report, but certainly does not meet STEMI criteria and is therefore an NSTEMI by definition. For national registry purposes, this will be incorrectly classified as a STEMI.) Most STEMI have peak cTnI greater than 10.0. Large STEMI are approximately 30-80.
The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. The paramedic notes called STEMI into question: “EMS disagree with monitor for STEMI callout. Do either, both, or neither have occlusion MI? Vitals were normal.
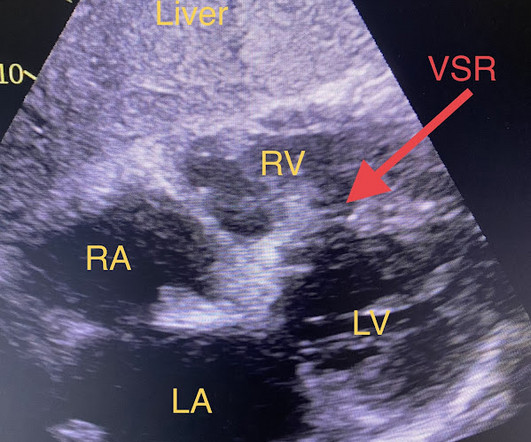
The conventional machine algorithm interpreted this ECG as STEMI. See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI. She was out walking her dog when she developed sudden dizziness and light-headedness. When EMS found her, she was dyspneic and diaphoretic. Answer : Bedside ultrasound!
But because there was no new ST elevation, the ECG was signed off as “STEMI negative” and the patient waited to be seen. But the ECG still doesn’t meet STEMI criteria. It was therefore interpreted as “no STEMI” and the patient was treated with dual anti-platelets and referred to cardiology as “NSTEMI.” the cardiologist 5.
QOH versions 1 and 2 both say Not OMI, with high confidence, without any clinical context, despite the abnormal STE meeting STEMI criteria. The ST/T wave ratio ( ie, the ratio of ST elevation compared to T wave amplitude ) in lead V6 is well over 0.24 ( See My Comment in the June 8, 2022 post for more on this Ratio ).
So we activated the Cath Lab Angiogram: Impression and Recommendations: Culprit for the patient's anterior ST segment myocardial infarction and out of hospital V-fib cardiac arrest is a thrombotic occlusion of the mid LAD The first troponin returned barely elevated at 36 ng/L (URL = 35) In our study of initial troponin in STEMI, 26.8%
Unfortunately you can see that the conventional Zoll algorithm sees nothing even to suggest AMI, let alone STEMI. For review on how I apply the Mirror Test I devised — See My Comment in the September 21, 2022 post in Dr. Smith's ECG Blog ). = Really unusual to me that QOH V1 only has low confidence, but at least its correct.
Discharge Diagnosis was STEMI (The STE did not meet "criteria," so "OMI" would be better, but "STEMI" is far better than what this could have been called: NonSTEMI) Quotes from a note written by a really fine and knowledgable physician: "12-lead EKG was obtained initial 1 at time zero. He was ventilated with BVM on arrival.
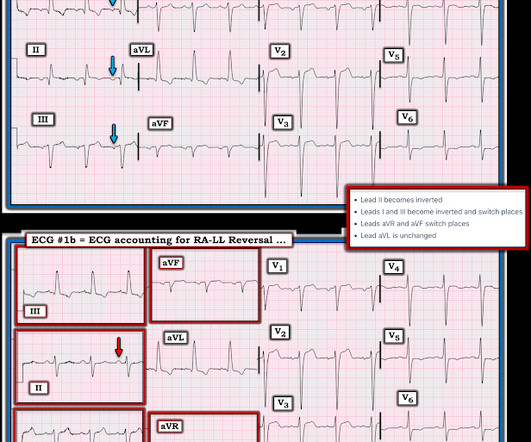
Here, I do not see OMI (although the ECG is falsely STEMI positive with just over 1 mm STE in V1 and about 2.5 The April 17, 2022 post ( Leads V1,V2 misplacement ). The May 5, 2022 post ( LA-RA reversal ). The May 24, 2022 post ( LA-LL reversal ). The May 26, 2022 post ( LA-LL reversal ). What do you think?
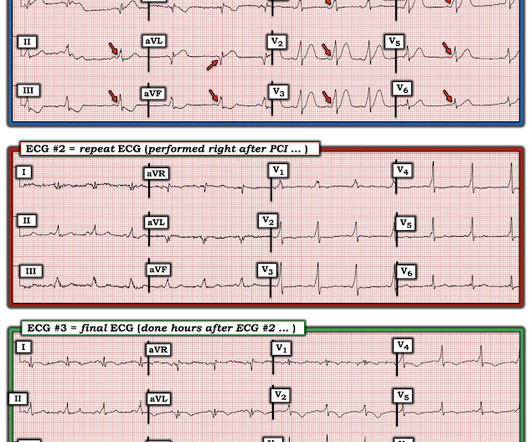
Here is the repeat ECG at 52 minutes after arrival to triage: Obvious posterolateral STEMI Angiographic findings: 1. 2022 ACC expert consensus decision pathway on the evaluation and disposition of acute chest pain in the emergency department: A report of the American college of cardiology solution set oversight committee. •
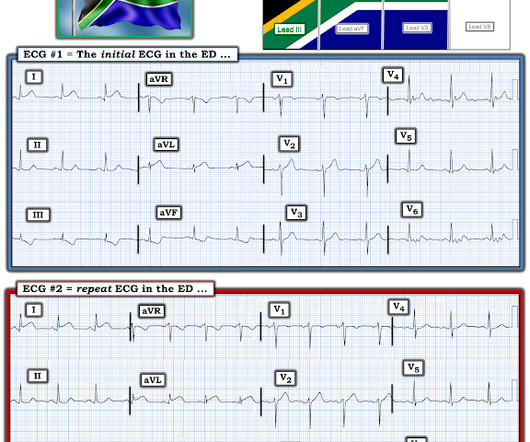
Here is the South African Flag sign ( Figure by Ken Grauer — with the original 12-lead from Patient 1 attached below — See his Comment from the April 8, 2022 post in Dr. Smith's ECG Blog for more on this sign ). ECG read as: "Shows T wave inversions in the inferior leads and less than 1mm STE in V2, without STEMI criteria."
She was diagnosed with a Non-STEMI and kept overnight for a next day angiogram. Medics recorded the above ECG and called a STEMI alert. Her symptoms at the time ECG #1 was obtained were CP and SOB — yet interpretation of this initial tracing prompted a STEMI alert. Her troponin I returned at 900 ng/L.
His EKG with worse pain now shows enough ST elevation to meet STEMI criteria. The EKG was read by the conventional computer algorithm as diagnostic of “ACUTE MI/STEMI”. The patient started receiving medications for “STEMI” (including heparin!!!) The ED provider canceled the STEMI protocol and updated the cath lab on the finding.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content