This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
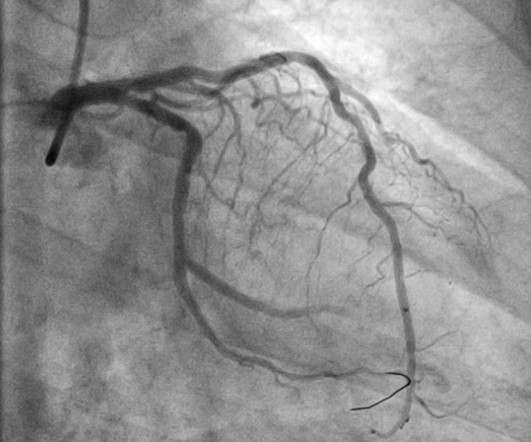
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. I would strongly consider the possibility of pure coronary spasm given the history, negative troponins and normal cath in light of the ECG changes seen below in Figure-1 ( See My Comment in the June 5, 2024 post by Dr. Nossen ).
Then assume there is ACS. Cardiac arrest #3: ST depression, Is it STEMI? or is he an ACCESS Trial Candidate? == MY Comment , by K EN G RAUER, MD ( 7/5 /2024 ): == Clinical ECG interpretation is a 2-Step process. The ST depression usually resolves, or is clearly resolving (getting much better).
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
There were zero patients in this study with a "normal" ECG who had any kind of ACS! So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. The patient was admitted as ‘NSTEMI’ which is supposed to represent a non-occlusive MI, but the underlying pathophysiology is analogous to a transient STEMI. Deutch et al.
Written by Bobby Nicholson What do you think of this “STEMI”? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). With EMS, patient had a GCS of 3 and was saturating 60% on room air. Version 2 = 0.0272.
While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. This case is an example of the steps we can all take in daily practice as the paradigm shifts from STEMI to OMI.
Smith : there is some minimal ST elevation in V2-V6, but does not meet STEMI criteria. Transient STEMI has been studied and many of these patients will re-occlude in the middle of the night. No wall motion abnormality This shows that significant ACS can have ZERO WMA!! Is it normal STE? This is a "Transient OMI". Am J Cardiol.
The emergency physician asked the advice of Dr. Reiters because of absence of STEMI criteria. The app also states that there is "suspected" ACS without ST elevation (NSTEMI), posterior fascicular block, sinus bradycardia, and LVH) Note on version 1 of the Queen: she will diagnose "OMI" whether it is an active or reperfused OMI.
Discharge ECG showed antero-inferior reperfusion T wave inversion: Had the initial ECG been signed off as “STEMI negative” the patient could have arrested in the waiting room, with a poor cardiac and neurological outcome. First trop was 90 ng/L (normal <16 in females) and peak was 7,400 ng/L.
Thus, these troponins are very concerning for ACS, and subsequent ones will probably be diagnostic of acute MI. Sometimes it can take 12 or 24 hours to see ECG evidence of reperfusion. == MY Comment , by K EN G RAUER, MD ( 1/4/ 2024 ): == Superb and thorough discussion by Dr. Frick of today's case! of the time.
The ECG was read as "No STEMI" and the patient was treated like an average chest pain patient (despite the fact that a chest pain patient with active pain and active subendocardial ischemia is very high risk). In our opinion it should not be given in ACS unless you are committed to the cath lab. It is already approved in Europe.
Because the most severe LAD OMIs can cause ischemic failure of the RBB and LAF, any patient with ACS symptoms and new RBBB and LAFB with any concordant STE has LAD OMI until proven otherwise. There is no recognition of STEMI equivalency in this setting in the USA guidelines currently. Long term outcome is unavailable.
The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Similarly, the OMI paradigm respects ACS as a dynamic process in which ECG changes reflect the phase of myocardial injury and risk stratify which patients may benefit from emergent PCI. Is there STEMI? What is the rhythm?
for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." Accessed May 28, 2024. showed that , when T-waves are inverted in precordial leads, if they are also inverted in lead III and V1, then pulmonary embolism is far more likely than ACS.
Background: ST-segment elevation myocardial infarction (STEMI) is a critical condition requiring rapid diagnosis and intervention. While ECGs play a central role in detecting STEMI, misinterpretations often occur, leading to unnecessary catheterization or missed diagnoses. Paper: Lee SH, Jeon KL, Lee YJ, Ko YG, Choi D, Hong MK, et al.
The is very small STE in III and aVF which do not meet STEMI criteria, hyperacute T waves, reciprocal TWI in aVL, and maximal STD in V2-V3 showing posterior OMI. The ECG was transmitted to the Emergency Medicine physician who recognized inferior and posterior OMI findings, and confirmed that the patient has potential ACS symptoms.
This dynamic change is diagnostic of ACS. Cardiology was consulted and agreed that his history was high risk for ACS and a next-day angiogram was merited. This was also non-diagnostic for OMI, although the dynamic changes are diagnostic of ACS. ECG at time 82 minutes: What do you think?
They recorded this ECG: Obvious inferior STEMI/OMI What else? The EMS ECGs: As per Dr. Smith the diagnosis of acute inferior STEMI is obvious from the history of new, severe CP in a patient with the initial EMS ECG that I show below ( TOP tracing in Figure-1 ). He called 911. Medics recorded a BP of 79/52 with pulse of 47.
However, due to the nature of the symptoms, the patient was treated for ACS and admitted to the hospital. Smith comment: Approximately 33% of cases that everyone would call STEMI reperfuse spontaneously (TIMI-1, 2, 3 flow) before they undergo emergent angiogram (usually under 90 minute door to balloon time) 20% have TIMI-3 flow.
Negative trops and negative angiogram does not rule out coronary ischemia or ACS. It is correct that he did not have chest pain, but we must remember that fully 1/3 of full blown STEMI do not present with chest pain. This is extremely elevated for a type 2 MI and totally consistent with STEMI. See these posts: Dynamic OMI ECG.
But thankfully, when the clinical context is clearly and highly concerning for ongoing ischemia from ACS, this distinction doesn't matter much. Final Diagnosis: "STEMI" (of course, as you can see in the ECGs above, this is not true, by definition this was NSTEMI. In other words, millimeters really don't matter! hours duration.
50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). Patients with suspected ACS should be evaluated with echocardiography. This correlates with potentially salvageable myocardium. See Raitt et al.:
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



























Let's personalize your content