This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
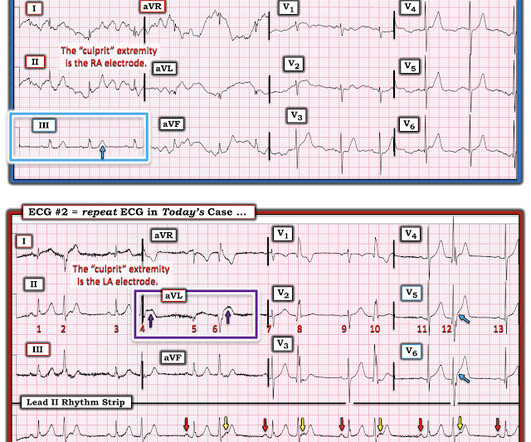
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
This was a machine read STEMI positive OMI. 118.007305) from Heitner et al. , The meaning of this quote is that at times, something as obvious as the dramatic anterior lead ST elevation that we see in today's tracing is not the result of an acute LAD STEMI. His ECG is shown below. Pretty obvious anterior current of injury.
The latest is Langlois-Carbonneau et al. If we took this as the gold standard, we would conclude that the computer interpretation was safe and accurate at least accurate enough to not miss STEMI, and that physicians should not be interrupted to interpret it, because there would be no change in patient management.
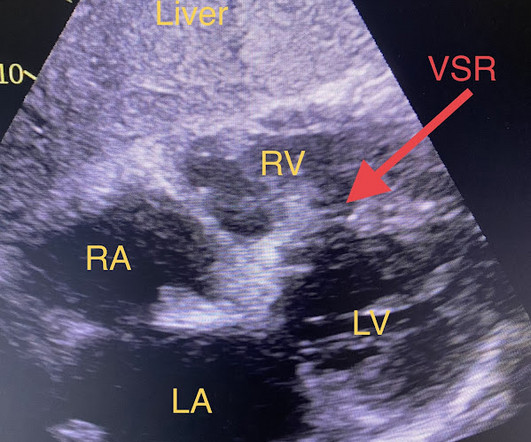
The conventional machine algorithm interpreted this ECG as STEMI. See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI. I've excerpted the Table shown below in Figure-2 from My Comment in that June 17, 2024 post. When EMS found her, she was dyspneic and diaphoretic.
So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. The patient was admitted as ‘NSTEMI’ which is supposed to represent a non-occlusive MI, but the underlying pathophysiology is analogous to a transient STEMI. Deutch et al. West J Emerg Med 2024).
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. Studies such as those by Moise et al 14 and Ellis et al 39 have shown that the relative risk of developing an acute myocardial infarction in the territory supplied by an artery with a 70%. He was started on nitro gtt.
The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. The paramedic notes called STEMI into question: “EMS disagree with monitor for STEMI callout. Vitals were normal except for oxygen saturation of 94%. Vitals were normal.
A Short Comment on PIRP and T Waves: Oliva et al found a strong association of myocardial rupture with postinfarction regional pericarditis. It has been estimated that in the aggregate, they occur at a rate of about 3 per 1000 patients with acute MI, and most of these events occur in patients with STEMI. Hammill SC. Edwards WD.
Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). As far as I can tell, there is only one randomized trial of immediate vs. delayed intervention for transient STEMI. Lemkes JS, et al.
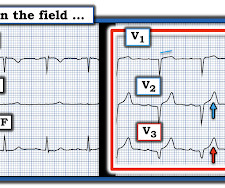
Smith : there is some minimal ST elevation in V2-V6, but does not meet STEMI criteria. Transient STEMI has been studied and many of these patients will re-occlude in the middle of the night. Lemkes et al. Is it normal STE? The computer thinks so, and the physician thinks that is quite possible. This is a "Transient OMI".
Heitner et al. Sometimes it can take 12 or 24 hours to see ECG evidence of reperfusion. == MY Comment , by K EN G RAUER, MD ( 1/4/ 2024 ): == Superb and thorough discussion by Dr. Frick of today's case! The PDA plaque was also bulky, but was not described as inflamed or ulcerated. DOI:10.1161/CIRCINTERVENTIONS.118.007305),
The ECG was read as "No STEMI" and the patient was treated like an average chest pain patient (despite the fact that a chest pain patient with active pain and active subendocardial ischemia is very high risk). The Queen of Hearts AI app will hopefully be FDA approved in Q1 of 2024. Hayakawa A, Tsukahara K, Miyagawa S, et al.
The limb leads have been removed because there was no ST elevation in those leads, the QRS complexes have been obscured because this is irrelevant to STEMI criteria, and red lines have been added to measure ST segment elevation. But STEMI criteria ignore all this and look at ST segments in isolation.
COACT: The COACT trial was fatally flawed, and because of it, many cardiologists are convinced that if there are no STEMI criteria, the patient does not need to go to the cath lab. Lemkes JS, Janssens GN, van der Hoeven NW, et al. These physicians did not want a patient with an OMI that was not a STEMI to be randomized to no angiogram.
The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Bigger et al. Is there STEMI? Sadowski ZP, Alexander JH, Skrabucha B, et al. Am Heart J 1999;137: 792–8 Alexander JH, Granger CB, Sadowski Z, et al, for the GUSTO-I and GUSTO-IIb Investigators. Leave it alone.
Microaxial Flow Pump or Standard Care in Infarct-Related Cardiogenic Shock Møller JE et al. DOI: 10.1056/NEJMoa2312572 Clinical Question In adults presenting with STEMI and cardiogenic shock does the use of a microaxial flow pump (Impella CP) compared to standard care reduce death from any cause at day 180?
This patient does not show up in the STEMI registry, and the time to reperfusion will likely not be identified as the problem that it was. The STEMI registry will show very high sensitivity of the ECG for STEMI, obscuring the fact the STEMI has low sensitivity for OMI Queen of Hearts sees it easily, like readers of the blog would.
for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." In fact, Kosuge et al. Accessed May 28, 2024. Stein et al. This is a paper worth reading : Marchik et al. Kosuge et al. Witting et al. of patients without PE.
It was read by the treating physician and the overreading cardiologist as "Paced, no STEMI." Lupu et al. As the troponin T was 1521 ng/L (peak troponin T over 1000 ng/L is typical of STEMI) and still rising, no further troponins were measured. How does the Queen of Hearts do? Clinical Cardiology. Curr Cardiol Rep [Internet].
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. In such cases — radiofrequency ablation of ectopic beats triggering malignant ventricular arrhythmias was needed for control of arrhythmic storm because the antiarrhythmic medications tried were ineffective ( Marrouche et al — JACC 5;43(9): 1715-20, 2004 ).
Unfortunately, the cardiologist waited until the next day to refer the patient for angiography and intervention because patient did not meet criteria for "STEMI"." And Olivier finishes with this commentary: "Yet another example in favor of abandoning STEMI criteria for diagnosing OMI. Peak troponin: 128,000 ng/L.
Background: ST-segment elevation myocardial infarction (STEMI) is a critical condition requiring rapid diagnosis and intervention. While ECGs play a central role in detecting STEMI, misinterpretations often occur, leading to unnecessary catheterization or missed diagnoses. Paper: Lee SH, Jeon KL, Lee YJ, Ko YG, Choi D, Hong MK, et al.
al in 2008, and is eponymously named after the main author. This ECG pattern is my favorite example of how the STEMI criteria are fundamentally flawed. We have a series of 20 TIMI-0 LAD Occlusions that do meet STEMI criteria. 2024, January 31). The ST-segment in lead V1 has upward convexity. 17 have HATW. Under Review.
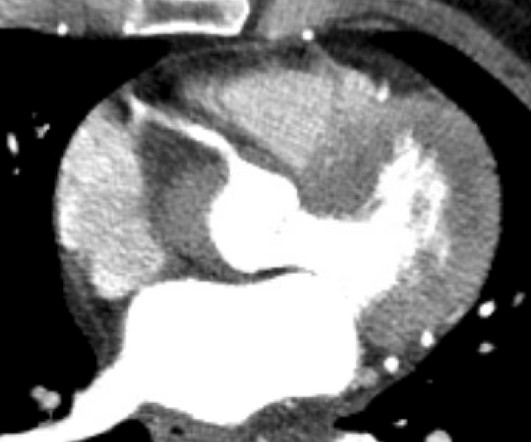
She had this ECG recorded: Obvious massive anterior STEMI She was quickly brought to the critical care area and the cath lab was activated. Here is the ECG at 25 minutes: Terrible LAD STEMI (+) OMI So a CT scan was done which of course showed a normal aorta. This time the Queen of Hearts interpreted: No STEMI or Equivalent.
Proving Cost Savings Our ED is a community Level II Trauma Center, Stroke Center, and STEMI [ST-elevation myocardial infarction] Receiving Center with 4,500 trauma activations, 569 hip fractures, and 450 rib fractures per year. Further questions can be directed to slamar1@rivhs.com References Hughes JA, Douglas C, Jones L, et al.
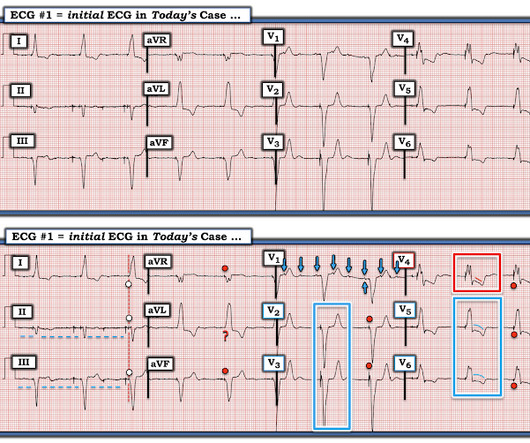
They recorded this ECG: Obvious inferior STEMI/OMI What else? The EMS ECGs: As per Dr. Smith the diagnosis of acute inferior STEMI is obvious from the history of new, severe CP in a patient with the initial EMS ECG that I show below ( TOP tracing in Figure-1 ). He called 911. Medics recorded a BP of 79/52 with pulse of 47.
It is diagnostic of OMI, but this is SUBACUTE OMI I sent this ECG to my "EKG Nerdz" friends, without any clinical info at all and they answered "OMI" The Queen said: "STEMI-Equivalent with High Confidence:" Notice she sees findings in both normal beats and PVCs. The November 8, 2024 post — artifact complicating OMI assessment.
The cath lab was deactivated by cardiologist on arrival at ED because it was "not a STEMI". Lupu et al. Reference : Lupu L, Taha L, Banai A, Shmueli H, Borohovitz A, Matetzky S, Gabarin M, Shuvy M, Beigel R, Orvin K, et al. Pt received 324 ASA and 2 sprays of nitro with improvement. Pain was decreased to 2/10.
See Raitt et al.: 50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). Oliva et al. [ This correlates with potentially salvageable myocardium. What should make you suspect PIRP? 4] Wang, S.,
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content