This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
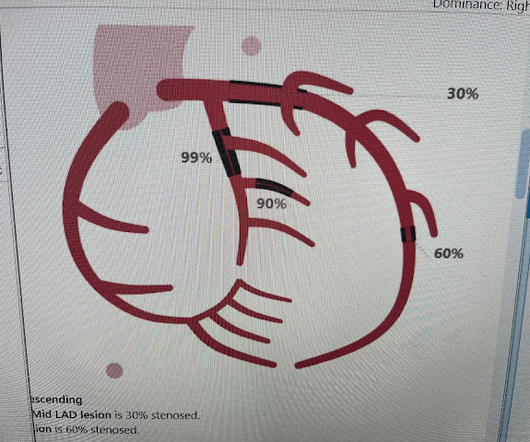
By Magnus Nossen This ECG is from a young man with no risk factors for CAD, he presented with chest pain. Before the lab values returned this patient had a n emergent coronary CT angiogram done that ruled out CAD. Each main coronary artery (LAD, RCA and LCx) are shown in separate images. There are no coronary stenoses.
The ECG is just a test: a Bayesian approach to acute coronary occlusion If a patient with a recent femur fracture has sudden onset of pleuritic chest pain, shortness of breath, and hemoptysis, the D-dimer doesn’t matter: the patient’s pre-test likelihood for PE is so high that they need a CT. Int J Cardiol 2024 3. Amsterdam et al.
The patient was treated as possible NSTEMI and underwent coronary angiography about 4 hours after presentation. TIMI 3 means the rate of passage of dye through the coronary artery is normal by angiography.) Initial hsTnI was 384 ng/L. The report describes a 60% proximal LAD lesion with TIMI 3 flow.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. The Queen of Hearts AI app will hopefully be FDA approved in Q1 of 2024. I have not yet seen any case report of this combination.
The ED provider ordered a coronary CT scan to assess the patient for CAD. The patient was taken emergently to the cath lab for a pericardiocentesis instead of a coronary angiogram. Three months prior to this presentation, he received a pacemaker for severe bradycardia and syncope due to sinus node dysfunction.
GLP-1 agonists are also associated with improved ejection fraction, coronary blood flow, and cardiac output while reducing the risk of cardiovascular events, infarction size, and all-cause mortality. Increased risk in those with preexisting CKD, other risk factors for renal disease (HTN or CAD), and those on ACEIs/ARBs.
Written by Pendell Meyers A woman in her 70s with known prior coronary artery disease experienced acute chest pain and shortness of breath. Her history and ECG were interpreted as very concerning for acute coronary syndrome which might benefit from acute reperfusion therapy. Vital signs were within normal limits. hours since onset.
No prior similar symptoms or known CAD. post OMI with significant multi-vessel coronary disease. He took two full strength aspirin prior to EMS arrival. The pain was relieved by one prehospital NTG spray. He arrived at the ED just shy of two hours after onset, pain free. PMHX significant for hypertension and BPH.
A 70-something dialysis patient presented and coronary disease had missed dialysis and then presented with acute onset of shortness of breath. Negative trops and negative angiogram does not rule out coronary ischemia or ACS. I was reading ECGs on the system and saw all of these, from one patient. He denied chest pain.
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergency department with chest pain. He looked back in time in the patient's chart and saw these ECGs and immediately recognized that they manifested subtle OMI. He had an EKG recorded right away.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















Let's personalize your content