This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Similarly, if a patient with known CAD presents with refractory ischemic chest pain, the ECG barely matters: the pre-test likelihood of acute coronary occlusion is so high that they need an emergent angiogram.
The ED provider ordered a coronary CT scan to assess the patient for CAD. His EKG with worse pain now shows enough ST elevation to meet STEMI criteria. The EKG was read by the conventional computer algorithm as diagnostic of “ACUTE MI/STEMI”. The patient started receiving medications for “STEMI” (including heparin!!!)
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. The Queen of Hearts AI app will hopefully be FDA approved in Q1 of 2024. I have not yet seen any case report of this combination.
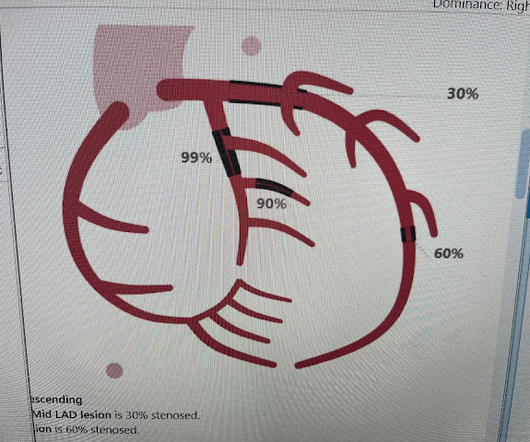
Scattered other nonobstructive CAD. This patient does not show up in the STEMI registry, and the time to reperfusion will likely not be identified as the problem that it was. Angiogram around 9am: Culprit lesion mid LAD 100% stenosis TIMI 0 TIMI 3 after PCI Severe apical dyskinesis, severe anteroapical akinesis.
The procedure was described as very complex due to severe multivessel CAD, but ultimately PCI was successfully performed to the ostial LCX. Final Diagnosis: "STEMI" (of course, as you can see in the ECGs above, this is not true, by definition this was NSTEMI. This ECG is taken from the July 25, 2024 post in Dr. Smith's ECG Blog.
No prior similar symptoms or known CAD. The Queen of Hearts Diagnosed "STEMI/STEMI equivalent" on that first ECG (she now uses "STEMI Equivalent" rather than OMI). The fact that she states "STEMI-Equivalent" here means that she does not think it is reperfused, but she does not know that the patient is pain free now.
It is correct that he did not have chest pain, but we must remember that fully 1/3 of full blown STEMI do not present with chest pain. This is extremely elevated for a type 2 MI and totally consistent with STEMI. As per Dr. Smith the Troponin peak of 16,000 is much more suggestive of a STEMI than of a Type II MI.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













Let's personalize your content