This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Thanks in part to rapid bedside diagnosis, the patient was able to avoid emergent coronary angiography. Here is lead I from ECGs 1 and 2 shown side-by-side to highlight the change in axis from borderline right to completely normal. While not completely ruling out acute coronary disease — another cause should be considered.
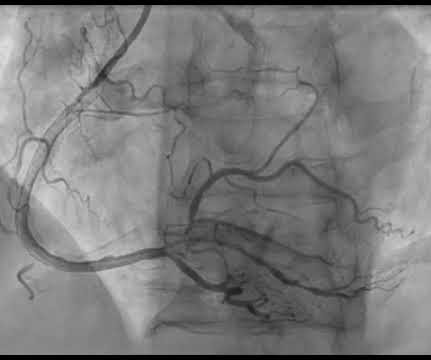
Coronaries were clean. I agree, however: 1) I don't think you can get a good enough ech o without bubble contrast. 3) E cho is another step that takes time. I agree, however: 1) I don't think you can get a good enough ech o without bubble contrast. 3) E cho is another step that takes time. Time is myocardium.
A 70-year-old female with a past medical history of hypertension, coronary artery disease s/p 2x drug eluting stent placement one month ago, atrial fibrillation on apixaban presents to the ED with weakness and lightheadedness. 1 Risk Factors: 1-4 Spontaneous Anticoagulants (Apixaban, Rivaroxaban, etc.)
We who know ischemic ECGs know that really when T-wave inversion is specific for coronary thrombosis that it indicates reperfusion of the artery, not active occlusion. Learning Point: 1. The Queen of Hearts AI app will hopefully be FDA approved in Q1 of 2024. Figure-1: Comparison between the first 3 ECGs in today's case.
Easy LINK — [link] — My New E CG P odcasts ( 5/28/2024 ): These podcasts are part of the Mayo Clinic Cardiovascular CME Podcasts Series ( "Making Waves" ) — hosted by Dr. Anthony Kashou. 0:00 — Intro by Dr. ) — published by Mayo Clinic CV Podcast Series on 1/16/2024 ( 33 minutes ). 9:25 — Are there hyperacute T waves?
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. C Examination notable for diaphoresis, 1+ bilateral lower extremity edema, regular heart rate and rhythm, and no signs of respiratory distress with normal breath sounds. Accessed May 28, 2024. What do you think? Stein et al.
1 The ED is a fast-paced environment where patient stability and life-and-limb-threatening conditions are prioritized. The pain began abruptly 1 hour ago, described as a stabbing sensation, and has occurred daily at the same time for the past week, each episode lasting about 45 minutes. Pain can be improved or exacerbated with meals.
Beats 1-2 and 7-10 are wider, uniform, and regular. I doubt retrograde conduction because the RP interval is variable between 8 and 9. If interested, you can review the angiography in detail on my coronary angiography guide where you will find a lot more information about coronary angiography generally.
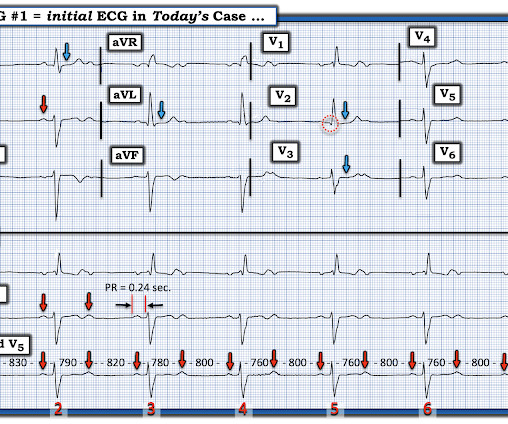
The ECG shows sinus rhythm with a rate of about 78 and 2:1 AV conduction along with right bundle branch block and left anterior fascicular block. 2:1 block is a special case, because the tracing lacks successive PR intervals. I have labeled the P waves below for ease of reference: P waves 8 and 9 both conduct to the ventricles.
Although these autoantibodies may be present in a variety of individuals, the development of clinical disease is thought to require exposure to an environmental risk factor such as certain viruses, cigarette smoke or other environmental toxins (1). million have been diagnosed with lupus, with 90% of cases occurring in females (1).
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















Let's personalize your content