This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
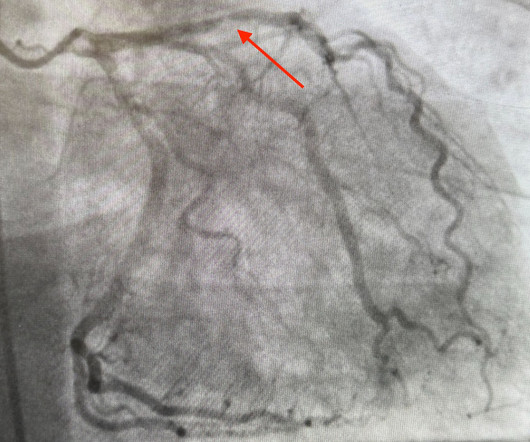
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergencydepartment with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. 2014 AHA/ACC guideline for the management of patients with non-ST elevation acute coronary syndromes.
1] But there are multiple other abnormalities that make this ECG diagnostic of Occlusion MI, localized likely to the right coronary artery: 1. Systematic review and meta-analysis of diagnostic test accuracy of ST-segment elevation for acute coronary occlusion. Int J Cardiol 2024 2. Eur Herat J Digital Health 2024
But like many similar studies, the study was small (one year at one centre with no indication of the incidence of acute coronary occlusion), and it used as the gold standard the final cardiologist interpretation of the ECG - not the patient outcome! Am J Emerg Med. Am J Emerg Med. Smith comment: this is even more stupid.
A man in his 90s with a history of HTN, CKD, COPD, and OSA presented to the emergencydepartment after being found unresponsive at home. Vital signs were within normal limits on arrival to the EmergencyDepartment. Am J Emerg Med. Written by Bobby Nicholson What do you think of this “STEMI”? or basilar ischemia.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergencydepartment with sudden onset weakness, fatigue, lethargy, and confusion. The undergraduate is now willing to identify himself: Hans Helseth. No ECG was ordered on Day #1.
, tells us that we physicians do not need to even look at this ECG until the patient is placed in a room because the computer says it is normal: Validity of Computer-interpreted “Normal” and “Otherwise Normal” ECG in EmergencyDepartment Triage Patients I reviewed this article for a different journal and recommended rejection and it was rejected.
Many systems now refrain from showing computer "normal" ECGs to the busy emergency physicians at triage because of very poorly conceived articles that say that if the computer algorithm says "normal," the emergency physician should not be bothered. It is clearly missed by the conventional algorithm.
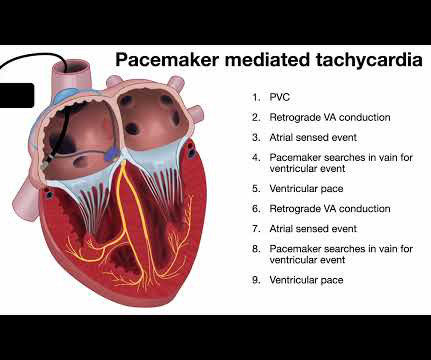
She presented to the emergencydepartment after a couple of days of chest discomfort. The patient is an older woman with known coronary disease and an ICD-Pacemaker implanted because of a history of VT ( V entricular T achycardia ). The last echocardiography 12 months ago showed HFmrEF. The ECG below was recorded.
2, 3 Biliary POCUS can help decrease patient length of stay in the EmergencyDepartment. Video 3: Coronary approach to the gallbladder POCUS Findings Sonographically, the gallbladder is situated in the right upper quadrant as an elongated pear-shaped organ on the inferior surface of the liver. J Educ Teach Emerg Med.
Date: September 23, 2024 Reference: Essat et al. Annals of Emergency Medicine, May 2024 Guest Skeptic: Dr. Casey Parker is a Rural Generalist from Australia who is also an ultrasounder. The patient has no specific risk factors for acute coronary syndrome (ACS) or dissection. Reference: Essat et al.
The ST segment changes are compatible with severe subendocardial ischemia which can be caused by type I MI from ACS or potentially from type II MI (non-obstructive coronary artery disease with supply/demand mismatch). The patient was rushed to the nearest emergencydepartment (non-PCI facility) for stabilization.
Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergencydepartment for evaluation of chest pain. 4) Lastly, the QRS amplitude in V2 (both the R- and S- waves) are measured.
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergencydepartment with 2 days of heavy substernal chest pain and nausea. Serial ECGs enhance the diagnosis of acute coronary syndrome. Annals of Emergency Medicine , 31 (1), 3–11. link] Fesmire, F.
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the EmergencyDepartment via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. Accessed May 28, 2024. What do you think? Labs obtained and notable for an elevated troponin I to 0.10
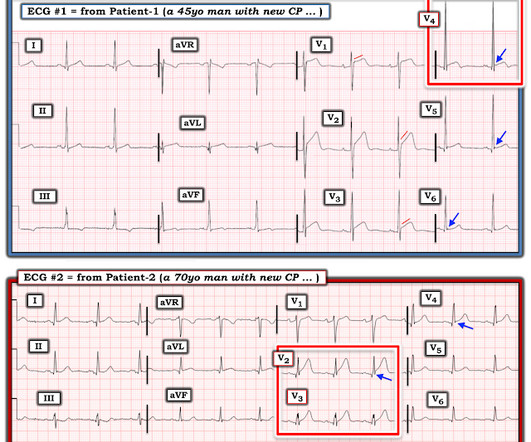
Using the current paradigm, can you tell which patient had an acute coronary occlusion? STEMI vs OMI Now let’s see the rest of the ECG: can you tell which patient has an acute coronary occlusion, and which ECG has hyperacute T waves? Using T wave amplitude, can you tell which ECG has hyperacute T waves? J Electrocardiol 2017 2.
54 It is vital to consider dangerous epigastric pain mimickers like acute coronary syndrome (ACS), hepatobiliary disease, or pancreatitis. The Treatment of Acute Pain in the EmergencyDepartment: A White Paper Position Statement Prepared for the American Academy of Emergency Medicine. J Emerg Med. Acad Emerg Med.
A very Merry Christmas from the BW team, and all the Best Wishes for 2024! Data was collected at 2 emergencydepartments in America and included assessment by both clinicians and patients for a total of 31 patients. Wounds are a common presentation to both adult and paediatric emergencydepartments.
And, finally, patients with a history of COPD frequently present to the emergencydepartment with dyspnea. Although dyspnea in this setting likely represents an AECOPD, other emergent differentials must be considered. ECG evaluates for dysrhythmias, acute coronary syndrome, or signs of right heart strain. Ann Emerg Med.
Annals of Emergency Medicine. PMID: 39066765 What They Did: The study involved the development of a deep ensemble AI model using ECG data from a prospective percutaneous coronary intervention registry in Korea. Development of Clinically Validated Artificial Intelligence Model for Detecting ST-segment Elevation Myocardial Infarction.
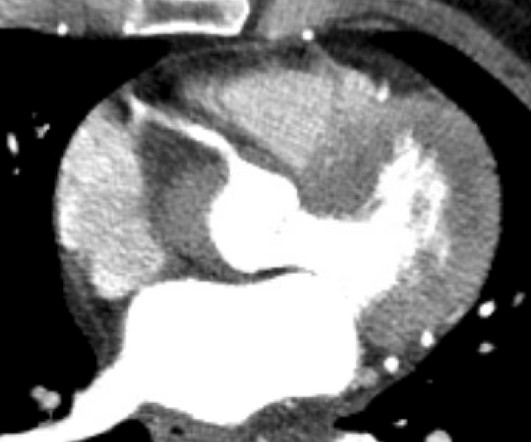
Cardiology wanted a CT of the aorta to rule out dissection, presumably partly due to the very high blood pressure readings, but also because it is hard for people to believe that a 20-something woman could have acute thrombotic coronary artery. Coronary malperfusion due to type A aortic dissection: mechanism and surgical management.
Written by Willy Frick with edits by Ken Grauer An older man with a history of non-ischemic HFrEF s/p CRT and mild coronary artery disease presented with chest pain. The following ECG was obtained in the emergencydepartment during active chest pain. He said he had had three episodes of chest pain that day while urinating.
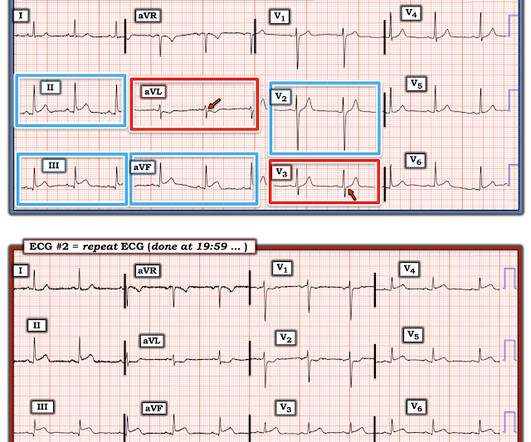
EMS gave aspirin and nitroglycerin, and the patient noted significant improvement on arrival to the EmergencyDepartment. My Comment , by K EN G RAUER, MD ( 11/10 /2024 ): = Think of today's case as a check of your skill in recognizing when to activate the cath lab. Why did the Repeat ECG look Better than ECG #1?
Case A 68 year old man with a medical history of hypertension, hyperlipidemia, and CAD with stent deployment in the RCA presented to the emergencydepartment with chest pain. Also : See Ken Grauer's excellent comments at the bottom. He developed it only 20 minutes prior to presentation while cutting branches outside.
SLE is considered an atypical risk factor for cardiovascular disease and acute coronary syndrome(8,9,11). Published 2024 Jan 2. PMID 37827694 The post Systemic Lupus Erythematosus: ED presentations, evaluation, and management appeared first on emDOCs.net - Emergency Medicine Education. Ann Rheum Dis. 2024;83(1):15-29.
The other important moment to always think of the heart (sorry, cardiologists, I don’t think about the heart 24/7) is when a collapsed neonate presents to your emergencydepartment, especially if blood pressure is present. This is one of the situations where you must not forget to feel for femoral pulses. L., & Carcillo, J.
Written by Pendell Meyers A woman in her 70s with known prior coronary artery disease experienced acute chest pain and shortness of breath. She presented to the EmergencyDepartment at around 3.5 She was emergently transferred to a PCI center. KEY Points: DSI does not indicate acute coronary occlusion!
He presented to the emergencydepartment for evaluation. Rates of occurrence of PIRP have decreased drastically in the era of percutaneous coronary intervention. Incidence and Prognosis of Pericarditis After ST-Elevation Myocardial Infarction (from the Acute Coronary Syndrome Israeli Survey 2000 to 2013 Registry Database).
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

























Let's personalize your content