This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
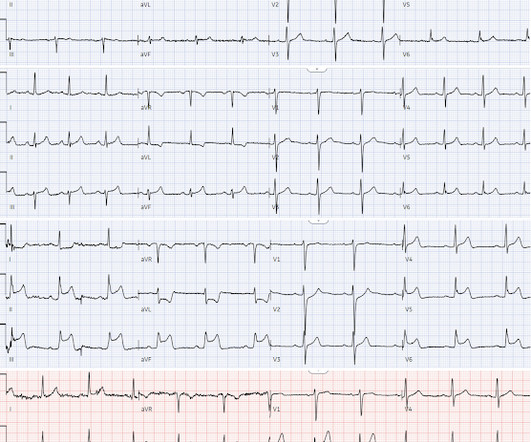
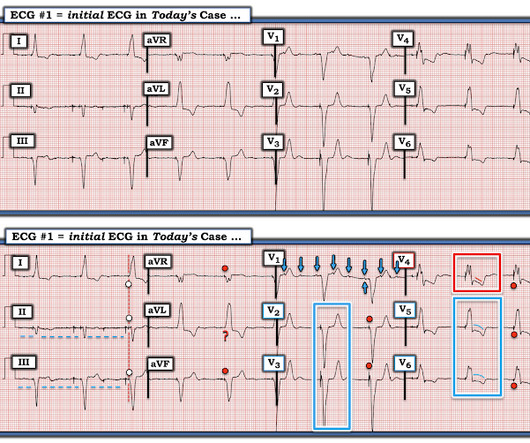
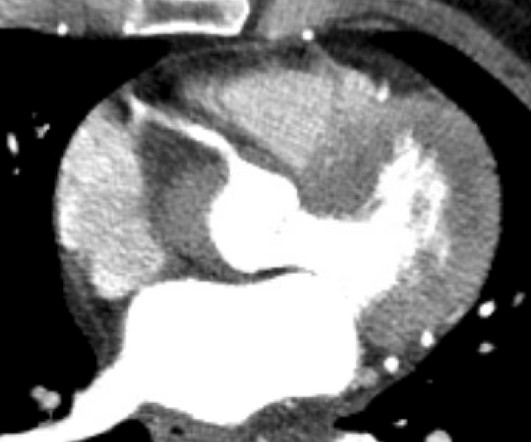
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. Compensatory enlargement was defined as being present when the total coronary arterial cross-sectional area at the stenotic site was greater than that at the proximal nonstenotic site. He was started on nitro gtt.
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Similarly, if a patient with known CAD presents with refractory ischemic chest pain, the ECG barely matters: the pre-test likelihood of acute coronary occlusion is so high that they need an emergent angiogram.
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
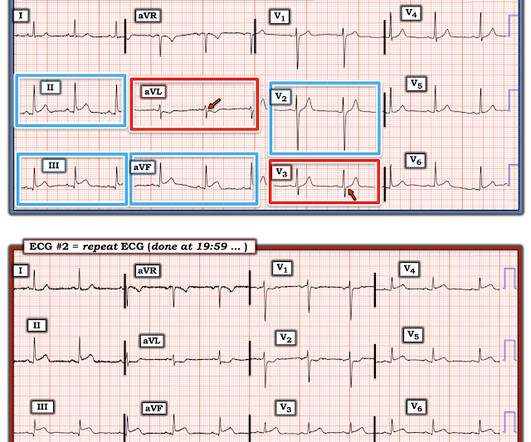
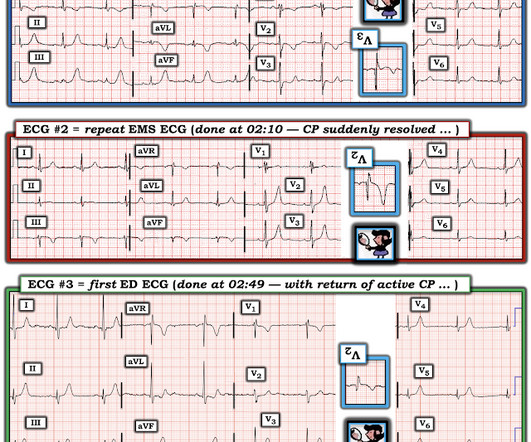
Obvious infero-postero-lateral STEMI(+)OMI, regardless of context Now let’s put them in order: what was the sequence? When the pain recurred the ECG normalized(ECG#2), but this is pseudonormalization : the coronary artery has spontaneously reoccluded, and the T waves are on their way up. What was the outcome and final diagnosis?
This certainly looks like an anterior STEMI (proximal LAD occlusion), with STE and hyperacute T-waves (HATW) in V2-V6 and I and aVL. How do you explain the anterior STEMI(+)OMI immediately after ROSC evolving into posterior OMI 30 minutes later? This caused a type 2 anterior STEMI.
So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
But cardiac arrest is a period of near zero flow in the coronary arteries and causes SEVERE ischemia. Cardiac arrest #3: ST depression, Is it STEMI? or is he an ACCESS Trial Candidate? == MY Comment , by K EN G RAUER, MD ( 7/5 /2024 ): == Clinical ECG interpretation is a 2-Step process. And what do you want to do?
But like many similar studies, the study was small (one year at one centre with no indication of the incidence of acute coronary occlusion), and it used as the gold standard the final cardiologist interpretation of the ECG - not the patient outcome! Despite serial ECGs being "STEMI negative", the cath lab was activated.
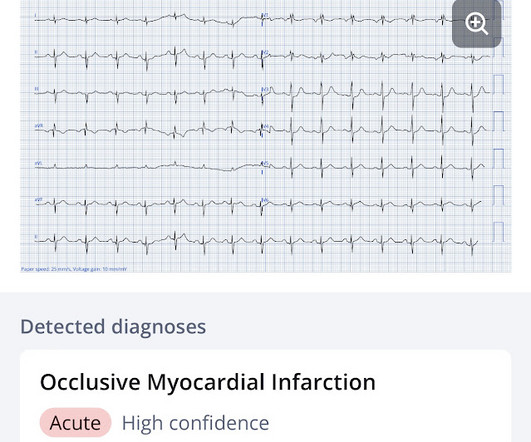
2024 Jan;75:137-142. 2024 Jan;22(1):140-151. 3: New AI-Powered OMI Detector Spoon Feed An artificial intelligence (AI) ECG model outperformed standard STEMI criteria in identifying occlusion myocardial infarction (OMI) confirmed by coronary angiography. Source High risk and low prevalence diseases: Infected urolithiasis.
The conventional machine algorithm interpreted this ECG as STEMI. See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI. Thanks in part to rapid bedside diagnosis, the patient was able to avoid emergent coronary angiography. When EMS found her, she was dyspneic and diaphoretic.
While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. This case is an example of the steps we can all take in daily practice as the paradigm shifts from STEMI to OMI.
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. West J Emerg Med 2024). Deutch et al.
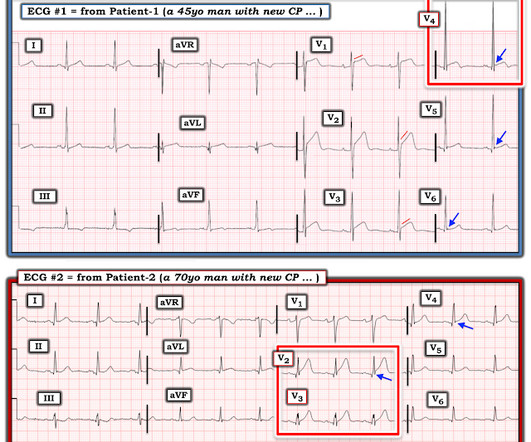
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. Additionally, his cardiac telemetry monitor showed runs of accelerated idioventricular rhythm, a benign arrhythmia often associated with coronary reperfusion.
Written by Bobby Nicholson What do you think of this “STEMI”? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). With EMS, patient had a GCS of 3 and was saturating 60% on room air. ng/mL and 0.10
Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). A comparison of electrocardiographic changes during reperfusion of acute myocardial infarction by thrombolysis or percutaneous transluminal coronary angioplasty.
Now it is a full blown STEMI of 3 myocardial territories: inferior, posterior, and lateral But at least it does not call it "Normal." Learning Points: You cannot trust conventional algorithms even to find STEMI(+) OMI, even when they say "normal ECG." It is clearly missed by the conventional algorithm.
Subtle as a STEMI." (i.e., Here is the bottom line of the article: It is widely believed that hyperacute T-waves are a transitional state preceding ST Elevation 1–4 Thus, it is tempting to postulate that early cases of OMI will eventually evolve to STEMI; yet, our data contradicts that notion. This one is easy for the Queen.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergency department with sudden onset weakness, fatigue, lethargy, and confusion. At 2111, the troponin I peaked at 12.252 ng/mL (this is in the range of STEMI patients, quite high). No ECG was ordered on Day #1.
The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. The paramedic notes called STEMI into question: “EMS disagree with monitor for STEMI callout. Coronaries were normal, as was serial troponin. Vitals were normal.
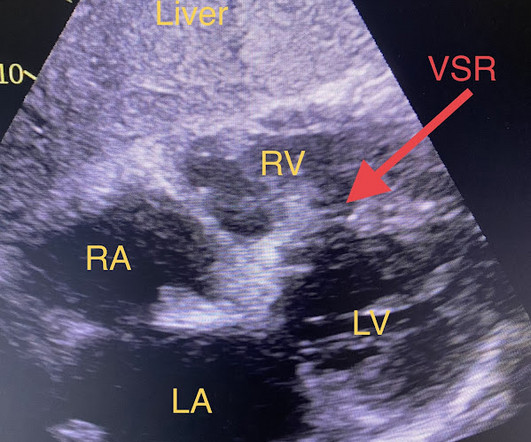
Another possible cause of pseudonormalization of T waves mentioned many times on this blog is the pseudonormalization caused by re-occlusion of an infarct related reperfused coronary artery. A mong patients with STEMI, ventricular septal rupture is the most common and free wall rupture is the least common. Hammill SC. Edwards WD.
Unfortunately you can see that the conventional Zoll algorithm sees nothing even to suggest AMI, let alone STEMI. Really unusual to me that QOH V1 only has low confidence, but at least its correct. During EMS transport, the pain suddenly resolved.
Smith : there is some minimal ST elevation in V2-V6, but does not meet STEMI criteria. Transient STEMI has been studied and many of these patients will re-occlude in the middle of the night. Is it normal STE? The computer thinks so, and the physician thinks that is quite possible. However , there is terminal QRS distortion in lead V3.
It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers. All coronary arteries were patent without atherosclerotic change. . == Below is the ECG of Patient #2 — as interpreted by the QOH. The ECG is diagnostic of occlusion myocardial infarction (OMI).
The ED provider ordered a coronary CT scan to assess the patient for CAD. His EKG with worse pain now shows enough ST elevation to meet STEMI criteria. The EKG was read by the conventional computer algorithm as diagnostic of “ACUTE MI/STEMI”. The patient started receiving medications for “STEMI” (including heparin!!!)
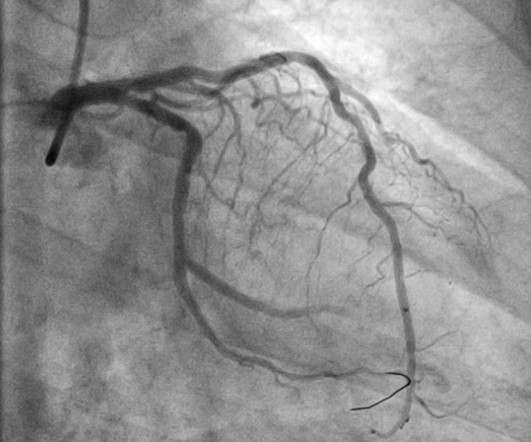
The Non-STEMI, which was an OMI, was diagnosed much faster with AI on the ECG than with troponin. For more on ECG findings in pulmonary disease — Check out My Comment in the May 31, 2024 post in Dr. Smith's ECG Blog ). The door to balloon time was incredibly short and there was a 100% circumflex occlusion that was opened and stented.
Here is the post shock ECG: Cardiology was called stat for ischemic VT, query SCAD vs thrombotic occlusion vs coronary vasospasm. Cath lab was activated: There was no coronary artery disease, but there was spontaneous coronary artery dissection (SCAD) of the distal LAD, which was narrowed by 95%, and treated medically.
Easy LINK — [link] — My New E CG P odcasts ( 5/28/2024 ): These podcasts are part of the Mayo Clinic Cardiovascular CME Podcasts Series ( "Making Waves" ) — hosted by Dr. Anthony Kashou. 2:25 — Dr. Grauer: The 1st Error : Too many clinicians in 2024 are still stuck in the outdated millimeter-based STEMI Paradigm”.
The ECG was read as "No STEMI" and the patient was treated like an average chest pain patient (despite the fact that a chest pain patient with active pain and active subendocardial ischemia is very high risk). The Queen of Hearts AI app will hopefully be FDA approved in Q1 of 2024. It is already approved in Europe. 2009;95:1701–1706.
Sometimes it can take 12 or 24 hours to see ECG evidence of reperfusion. == MY Comment , by K EN G RAUER, MD ( 1/4/ 2024 ): == Superb and thorough discussion by Dr. Frick of today's case! We know that even high-sensitivity troponin may not exceed the "normal" range for a period of hours in certain patients with acute coronary occlusion.
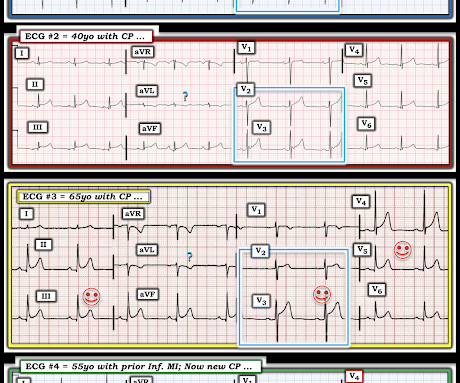
The limb leads have been removed because there was no ST elevation in those leads, the QRS complexes have been obscured because this is irrelevant to STEMI criteria, and red lines have been added to measure ST segment elevation. Using the current paradigm, can you tell which patient had an acute coronary occlusion?
The proof of this is that only 5% of patients enrolled had acute coronary occlusion. COACT: The COACT trial was fatally flawed, and because of it, many cardiologists are convinced that if there are no STEMI criteria, the patient does not need to go to the cath lab. This study failed to do so. 5% vs. 58%!!
This ECG is highly concerning for LAD occlusion despite it not showing a STEMI criteria. You can find the variables used to calculate the value on MD calc here: [link] Utilizing Dr. Smith’s Subtle Anterior STEMI Calculator (4-Variable), the value is greater than 18.2 which is concerning for LAD occlusion.
The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Serial ECGs enhance the diagnosis of acute coronary syndrome. Is there STEMI? Association of intravenous morphine use and outcomes in acute coronary syndromes: Results from the Crusade Quality Improvement Initiative.
It was read by the treating physician and the overreading cardiologist as "Paced, no STEMI." Immediate and early percutaneous coronary intervention in very high risk and high risk non-ST segment elevation myocardial infarction patients. How does the Queen of Hearts do? Lupu et al. Clinical Cardiology. Am Heart J [Internet].
"Unfortunately, the cardiologist waited until the next day to refer the patient for angiography and intervention because patient did not meet criteria for "STEMI"." The coronary angiography showed a 100% ostial main (obtuse) marginal occlusion!" Dominant right coronary, atherosclerotic and calcified. Peak troponin: 128,000 ng/L.
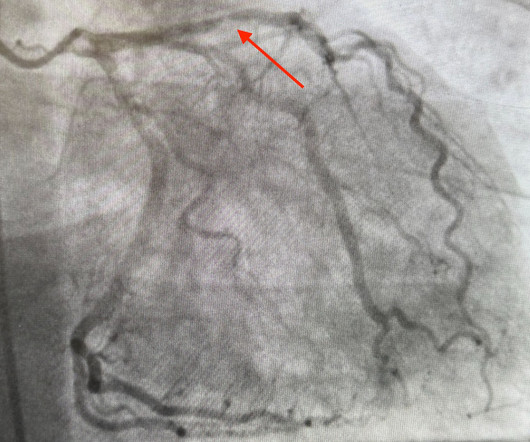
The ECG shows obvious STEMI(+) OMI due to probable proximal LAD occlusion. It shows a proximal LAD occlusion, in conjunction with a subtotally occluded LMCA ( Left Main Coronary Artery ). The patient in today’s case is a previously healthy 40-something male who contacted EMS due to acute onset crushing chest pain.
for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." Electrocardiographic Differentiation Between Acute Pulmonary Embolism and Acute Coronary Syndromes on the Basis of Negative T Waves - ScienceDirect. Accessed May 28, 2024.
Background: ST-segment elevation myocardial infarction (STEMI) is a critical condition requiring rapid diagnosis and intervention. While ECGs play a central role in detecting STEMI, misinterpretations often occur, leading to unnecessary catheterization or missed diagnoses. Paper: Lee SH, Jeon KL, Lee YJ, Ko YG, Choi D, Hong MK, et al.
Written by Jesse McLaren, with edits from Meyers Four patients presented with chest pain or shortness of breath, and ECGs labeled ‘inferior STEMI’. Less concavity associated with hyperacuity This can help identify false negative STEMI, or STEMI(-)OMI, at risk for delayed reperfusion. More asymmetry 3.
But it does not meet the ridiculous "STEMI criteria" since there is not 1 mm of STE in any lead. Learn to read the ECG for sublte OMI, and get the Queen of Hearts. == MY Comment , by K EN G RAUER, MD ( 11/1 /2024 ): == The beauty of today's case is its simple efficiency. So this is acute OMI. What does the Queen of Hearts say? (Dr.
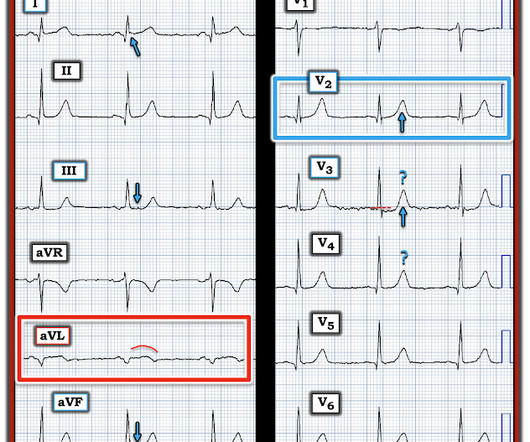
The is very small STE in III and aVF which do not meet STEMI criteria, hyperacute T waves, reciprocal TWI in aVL, and maximal STD in V2-V3 showing posterior OMI. The cath lab was activated despite lack of STEMI criteria, around 2 am in the morning. 33% of STEMI are reperfused by the time of angiography. Very frustrating.
She had this ECG recorded: Obvious massive anterior STEMI She was quickly brought to the critical care area and the cath lab was activated. Here is the ECG at 25 minutes: Terrible LAD STEMI (+) OMI So a CT scan was done which of course showed a normal aorta. This time the Queen of Hearts interpreted: No STEMI or Equivalent.
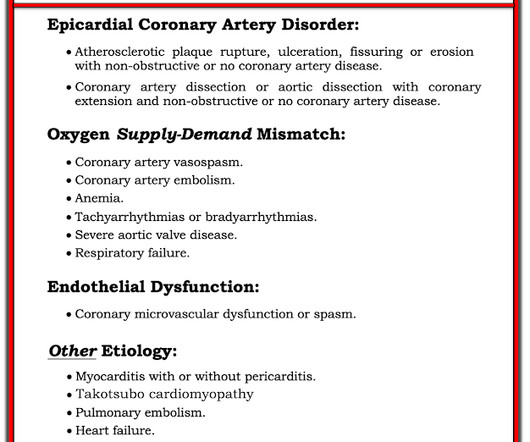
They recorded this ECG: Obvious inferior STEMI/OMI What else? Myocardial Infarction with Non-Obstructive Coronary Arteries. Etiologies (list not comprehensive): Coronary Spasm. For more on the ECG diagnosis and consequences of acute RV MI Check out My Comment in July 19, 2020 post and the August 2, 2024 post).
This ECG pattern is my favorite example of how the STEMI criteria are fundamentally flawed. We have a series of 20 TIMI-0 LAD Occlusions that do meet STEMI criteria. This typically occurs in the setting of a rapidly reperfused coronary artery following a myocardial infarction. 2024, January 31). 17 have HATW. Wellens, H.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content