This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
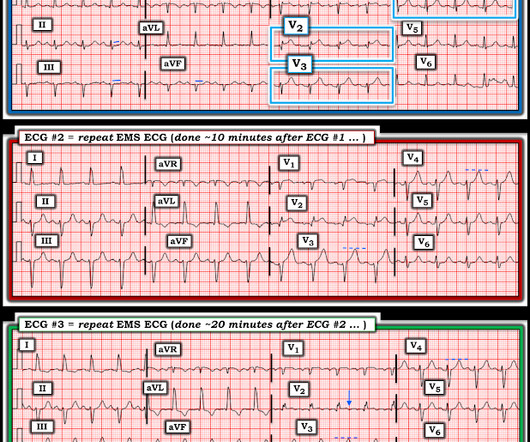
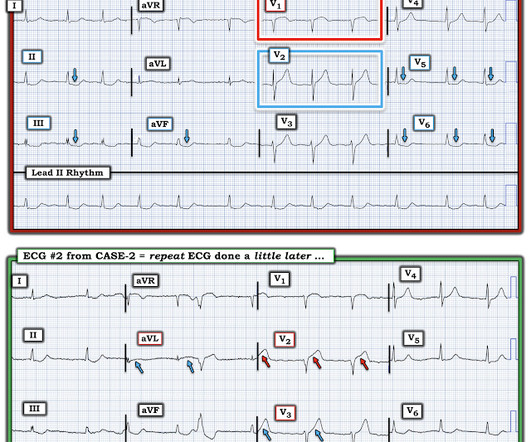
Interpretation : diagnostic of acute anterior OMI with STE less than STEMI criteria in V1-V4, hyperacute T waves in V2-V4, and suspiciously flat isoelectric ST segments in III and aVF suspicious for reciprocal findings. Now it even meets STEMI criteria, and HATWs continue to inflate. So the cath lab was not activated. Ongoing OMI.
He arrived to the ED with severe hypotension, heart rate in the 70s, unable to follow commands but moving all extremities requiring restraint and sedation, respiratory rate around 24/min being supported with bag valve mask, with significant hypoxemia. His family started CPR and called EMS, who arrived to find him in ventricular fibrillation.
From April 2-5, the top fire services and EMS industry thought leaders and data analysts gathered at Wave 2024 to share what trends they’re forecasting for both fields and how they’re enacting change within their own organizations through the power of data-driven insights. It’s four days of thought leadership, networking, and learning.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. He arrived to the ED by helicopter at 1507, about three hours after the start of his chest pain while chopping wood around noon. He wrote most of it and I (Smith) edited.
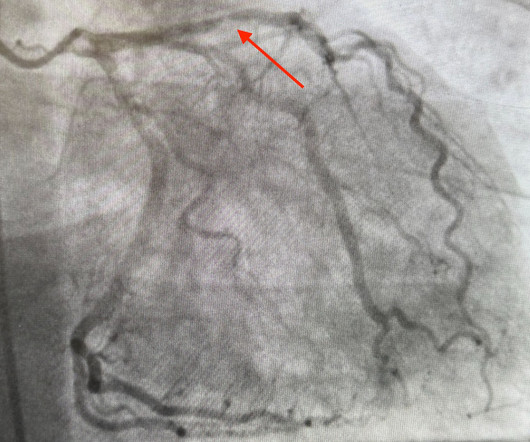
So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
This certainly looks like an anterior STEMI (proximal LAD occlusion), with STE and hyperacute T-waves (HATW) in V2-V6 and I and aVL. On arrival to the ED, this ECG was recorded: What do you think? How do you explain the anterior STEMI(+)OMI immediately after ROSC evolving into posterior OMI 30 minutes later?
So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. The patient was admitted as ‘NSTEMI’ which is supposed to represent a non-occlusive MI, but the underlying pathophysiology is analogous to a transient STEMI. West J Emerg Med 2024). Fortunately the patient did not reocclude while awaiting the angiogram.
Our data corroborate that immediate management of a patient with a normal automated triage ECG reading is not modified by real-time ED physician ECG interpretation." Smith comment: we showed that the first troponin, even in full-blown STEMI, is negative 25% of the time. But according to Langlois-Carbonneau et al.,
While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. It’s unclear if the paramedic ECGs were seen or missed in the ED. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. At this point the emergency physician asked for a stat cardiology consult.
. #1: How to Treat Infected Kidney Stones Spoon Feed All patients with infected ureteral stones necessitate a urine culture, antibiotics, and urology consultation in the ED, with the majority requiring admission for surgical intervention. 2024 Jan;75:137-142. 2024 Jan;22(1):140-151. Am J Emerg Med. doi: 10.1016/j.ajem.2023.10.049.
Written by Bobby Nicholson What do you think of this “STEMI”? EKG on arrival to the ED is shown below: What do you think? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). or basilar ischemia.
The conventional machine algorithm interpreted this ECG as STEMI. See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI. Consider the following: We become attuned to looking for acute coronary occlusion in patients who present with acute symptoms to the ED ( E mergency D epartment ).
Subtle as a STEMI." (i.e., Here is the bottom line of the article: It is widely believed that hyperacute T-waves are a transitional state preceding ST Elevation 1–4 Thus, it is tempting to postulate that early cases of OMI will eventually evolve to STEMI; yet, our data contradicts that notion. This one is easy for the Queen.
It was present on arrival at triage but then resolved before bed placement in the ED. Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). It is a ssociated with mild dyspnea on exertion. Aspirin given.
male presents to the ED at 6:45 AM with left sided chest dull pressure that woke him up from sleep at 3am. He arrived to the ED at around 6:45am, and stated the pain has persisted. Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. The pain radiated to both shoulders.
The patient was brought to the ED and had this ECG recorded: What do you think? Cardiac arrest #3: ST depression, Is it STEMI? or is he an ACCESS Trial Candidate? == MY Comment , by K EN G RAUER, MD ( 7/5 /2024 ): == Clinical ECG interpretation is a 2-Step process. After 1 mg of epinephrine they achieved ROSC.
Now it is a full blown STEMI of 3 myocardial territories: inferior, posterior, and lateral But at least it does not call it "Normal." Learning Points: You cannot trust conventional algorithms even to find STEMI(+) OMI, even when they say "normal ECG." At this point — a STEMI was diagnosed, and cardiac cath with PCI was performed.
Written by Jesse McLaren Two patients in their 70s presented to the ED with chest pain and RBBB. The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. Do either, both, or neither have occlusion MI? Vitals were normal.
ECG 1 at time zero EARLY REPOLARIZATION ABNORMAL ECG ED final official overread: "early repol vs hyperacute T, minimal changes from previous (previous shown below)" What do YOU think? Smith : there is some minimal ST elevation in V2-V6, but does not meet STEMI criteria. Is it normal STE? This is a "Transient OMI". Am J Cardiol.
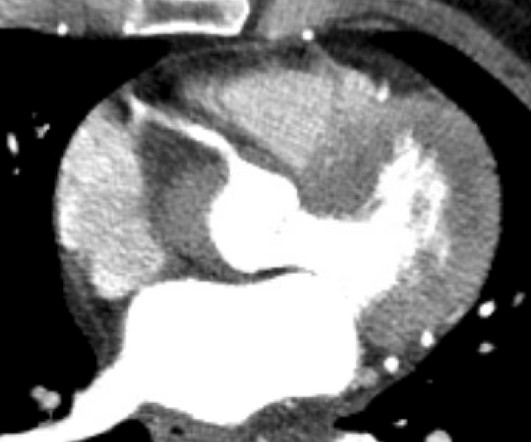
Case An 82 year old man with a history of hypertension presented to the ED with chest pain at 1211. The ED provider ordered a coronary CT scan to assess the patient for CAD. His pain suddenly became much worse in the ED and he became acutely diaphoretic, dizzy, and hypotensive. There is pericardial tamponade.
This patient had the onset of chest pain 24 hours before arrival to the ED. The Non-STEMI, which was an OMI, was diagnosed much faster with AI on the ECG than with troponin. For more on ECG findings in pulmonary disease — Check out My Comment in the May 31, 2024 post in Dr. Smith's ECG Blog ). It had never been described before.
Submitted by Dr. George Mastoras (Twitter @georgemastoras), written by Jesse McLaren It’s a busy day in the ED when you’re sent another ECG to sign off from a patient at triage. A healthy 45-year-old female presented with chest pain, with normal vitals. First trop was 90 ng/L (normal <16 in females) and peak was 7,400 ng/L.
Later, I found old ECGs: 5 month prior in clinic: V5 and V6 look like OMI 9 months prior in clinic with no chest symptoms: V5 and V6 look like OMI 1 year prior in the ED with chest pain: V5 and V6 sure look like a STEMI For this ECG and chest pain in the ED, the Cath lab activated. But the angiogram was clean. There was no OMI.
At 2111, the troponin I peaked at 12.252 ng/mL (this is in the range of STEMI patients, quite high). Consider the scenario in today's CASE: This 56-year old man with risk factors including diabetes and known coronary disease — presented to the ED on Day #1 with new weakness , fatigue , lethargy and confusion.
Another missed OMI by the False STEMI-NonSTEMI Dichotomy Don't miss them!!! BOTTOM Line for CASE #1: Prompt recognition of the precordial "Swirl" pattern of acute LAD OMI resulted in stent reperfusion in less than 90 minutes from the time of arrival in the ED. Use the Queen of Hearts and save myocardium and lives!
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. The Queen of Hearts AI app will hopefully be FDA approved in Q1 of 2024. I have not yet seen any case report of this combination.
The paramedic called the EM physician ahead of arrival and discussed the case and ECGs, and both agreed upon activating "Code STEMI" (even though of course it is not STEMI by definition), so that the acute LAD occlusion could be treated as fast as possible. So the cath lab was activated. Long term outcome is unavailable.
From April 2-5, ESO brought the hospital industry’s top thought leaders and data analysts together at Wave 2024 to share what trends they’re forecasting for the medical field along with how they’re enacting change within their own organization through the power of data-driven insights. ESO has resources to keep you informed.
Here was his initial ED ECG: Formal interpretation by interventional cardiologist: There is "Non-diagnostic" ST Elevation in V2-V4 and aVL. COACT: The COACT trial was fatally flawed, and because of it, many cardiologists are convinced that if there are no STEMI criteria, the patient does not need to go to the cath lab.
Cardiology refused to be the admitting physician because it was "NSTEMI", and forced the ED physician to admit the patient to the hospitalist. Of course, there was terrible boarding and the patient was considered non-emergent (NSTEMI), and so could not leave the ED for some time. YOU TOO CAN HAVE THE PM Cardio AI BOT!!
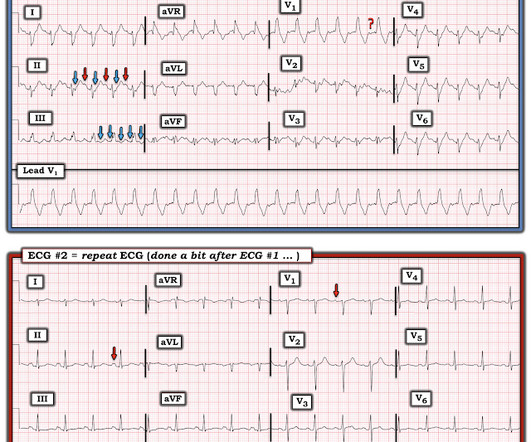
== MY Comment , by K EN G RAUER, MD ( 8/30 /2024 ): == I was sent the ECG shown in Figure-1 — knowing only that the patient was being seen in the ED ( E mergency D epartment ). 2 Informational: I was provided with a repeat ECG on this patient — which was recorded a bit after ECG #1, still in the ED ( Bottom tracing in Figure-3 ).
He reported typical chest pain since 4H AM and arrived at our ED at 10h with ongoing chest pain. Unfortunately, the cardiologist waited until the next day to refer the patient for angiography and intervention because patient did not meet criteria for "STEMI"." The first ECG (10h14) showed TWI in inferior leads."
for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." Accessed May 28, 2024. In 2024 — once the diagnosis of acute is contemplated, point of care Echo and/or CTPA ( C omputed T omography P ulmonary A ngiography ) enable expedited confirmation.
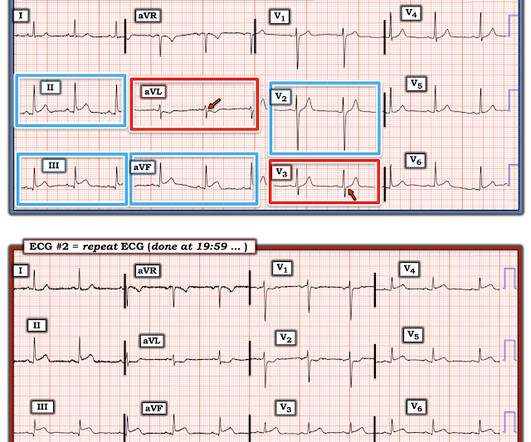
The is very small STE in III and aVF which do not meet STEMI criteria, hyperacute T waves, reciprocal TWI in aVL, and maximal STD in V2-V3 showing posterior OMI. The cath lab was activated despite lack of STEMI criteria, around 2 am in the morning. Here is her ECG on arrival to the ED: Improved, but still some signal of posterior OMI.
Background: ST-segment elevation myocardial infarction (STEMI) is a critical condition requiring rapid diagnosis and intervention. While ECGs play a central role in detecting STEMI, misinterpretations often occur, leading to unnecessary catheterization or missed diagnoses. Paper: Lee SH, Jeon KL, Lee YJ, Ko YG, Choi D, Hong MK, et al.
This was written by one of our fine residents, who will soon be an EMS fellow: Michael Perlmutter Case A mid-50s male came to the ED with a burning sensation that was acutely worse while at home. He came to the ED at the urging of his wife. Note also development of distinct J-point notching in leads V3 , V4 that was not seen earlier.
She had this ECG recorded: Obvious massive anterior STEMI She was quickly brought to the critical care area and the cath lab was activated. Here is the ECG at 25 minutes: Terrible LAD STEMI (+) OMI So a CT scan was done which of course showed a normal aorta. This time the Queen of Hearts interpreted: No STEMI or Equivalent.
He arrived at the ED just shy of two hours after onset, pain free. Here is the initial ED ECG: Here that first ECG is cleaned up by PM Cardio app: What do you think? The Queen of Hearts Diagnosed "STEMI/STEMI equivalent" on that first ECG (she now uses "STEMI Equivalent" rather than OMI).
Around the world, acute pain is the most common reason for patients to present to the emergency department (ED). We propose a novel concept for the implementation of a regional anesthesia service aimed at providing pain relief to both ED patients and those admitted to the hospital. link] Published June 17, 2024. Int Emerg Nurs.
Smith : I recognize this as a STEMI mimic. See here for young women with OMI == MY Comment , by K EN G RAUER, MD ( 12/24 /2024 ): == I found today's case challenging and an excellent example of how despite my not being certain of the diagnosis from the history and initial ECG careful follow-up yielded the answer. I was not alarmed.
They recorded this ECG: Obvious inferior STEMI/OMI What else? He arrived in the ED and had this ECG recorded: The first high sensitivity troponin I returned undetectable (3 ng/L). For more on the ECG diagnosis and consequences of acute RV MI Check out My Comment in July 19, 2020 post and the August 2, 2024 post). He called 911.
The ECG meets STEMI criteria objectively. The ED physician did not think the ECG represented OMI. One other ECG was obtained during the ED stay: The patient was discharged home. See My Comment in the June 25, 2024 post for changes with LA-LL reversal ). PM Cardio QOH says No signs of OMI. AMI was ruled out.
Queen : she saw no OMI (no "STEMI Equivalent") either Continued : Now, she says she was walking to the bathroom when she experienced acute onset substernal chest pressure radiating into her neck and left arm. Her ECG afterward is shown below: ECG from five days prior Smith : this shows an old inferior MI with persistent ST elevation.
He arrived in our ED with the below ECG pain free. All of these findings together makes this ECG diagnostic of inferior and posterior occlusion myocardial infarction (OMI) The patient is this case was treated as if he had an ongoing OMI. Primary PCI was not feasible and therefore the patient was given thrombolytics by EMS.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content