This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
. #1: Emergent Cath Lab Activations with “Normal” Computer ECG Interpretations Spoon Feed A significant minority of code STEMI patients have an initial normal computer ECG interpretation. Consequently, emergency physicians must remain vigilant to identify signs of OMI regardless of the initial computer ECG interpretation.
Source Use of Glucagon-Like Peptide-1-Agonists and Increased Risk of Procedural Sedation and Endotracheal Intubation in the EmergencyDepartment. Ann Emerg Med. 2024 Aug;84(2):226-227. Ann Emerg Med. 2024 Jul 25:S0196-0644(24)00327-5. 2024 Jul 1;154(1):e2023064364. DOI: 10.1016/j.annemergmed.2024.03.007.
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergencydepartment with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion.
If we took this as the gold standard, we would conclude that the computer interpretation was safe and accurate at least accurate enough to not miss STEMI, and that physicians should not be interrupted to interpret it, because there would be no change in patient management. What is the gold standard for ECG interpretation: patient outcome!!!
Written by Bobby Nicholson What do you think of this “STEMI”? A man in his 90s with a history of HTN, CKD, COPD, and OSA presented to the emergencydepartment after being found unresponsive at home. Vital signs were within normal limits on arrival to the EmergencyDepartment. Am J Emerg Med. ng/mL and 0.10
, tells us that we physicians do not need to even look at this ECG until the patient is placed in a room because the computer says it is normal: Validity of Computer-interpreted “Normal” and “Otherwise Normal” ECG in EmergencyDepartment Triage Patients I reviewed this article for a different journal and recommended rejection and it was rejected.
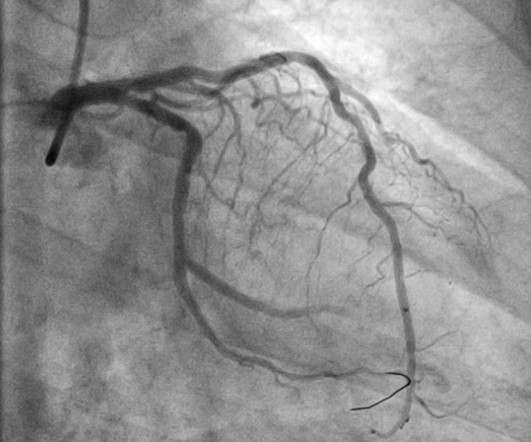
Now it is a full blown STEMI of 3 myocardial territories: inferior, posterior, and lateral But at least it does not call it "Normal." Learning Points: You cannot trust conventional algorithms even to find STEMI(+) OMI, even when they say "normal ECG." At this point — a STEMI was diagnosed, and cardiac cath with PCI was performed.
QOH versions 1 and 2 both say Not OMI, with high confidence, without any clinical context, despite the abnormal STE meeting STEMI criteria. Context: a man in his 40s presented to the emergencydepartment with 1 day of sudden onset chest pain. I sent this to our group without information and Dr. Smith responded: "Not OMI.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergencydepartment with sudden onset weakness, fatigue, lethargy, and confusion. At 2111, the troponin I peaked at 12.252 ng/mL (this is in the range of STEMI patients, quite high).
The limb leads have been removed because there was no ST elevation in those leads, the QRS complexes have been obscured because this is irrelevant to STEMI criteria, and red lines have been added to measure ST segment elevation. But STEMI criteria ignore all this and look at ST segments in isolation.
Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergencydepartment for evaluation of chest pain. which is concerning for LAD occlusion.
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergencydepartment with 2 days of heavy substernal chest pain and nausea. The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Is there STEMI?
Written by Pendell Meyers A man in his late 30s with history of hypertension, tobacco use, and obesity presented to the EmergencyDepartment for acute chest pain which started approximately 3 hours prior to arrival, in the setting of a very stressful situation. The pain radiated down both arms, 10/10 in severity.
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the EmergencyDepartment via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. Accessed May 28, 2024. What do you think? Labs obtained and notable for an elevated troponin I to 0.10
Background: ST-segment elevation myocardial infarction (STEMI) is a critical condition requiring rapid diagnosis and intervention. While ECGs play a central role in detecting STEMI, misinterpretations often occur, leading to unnecessary catheterization or missed diagnoses. Annals of Emergency Medicine.
Around the world, acute pain is the most common reason for patients to present to the emergencydepartment (ED). Identifying patients presenting in pain to the adult emergencydepartment: a binary classification task and description of prevalence. Int Emerg Nurs. link] Published June 17, 2024. 2019;12:59-66.
The is very small STE in III and aVF which do not meet STEMI criteria, hyperacute T waves, reciprocal TWI in aVL, and maximal STD in V2-V3 showing posterior OMI. The ECG was transmitted to the Emergency Medicine physician who recognized inferior and posterior OMI findings, and confirmed that the patient has potential ACS symptoms.
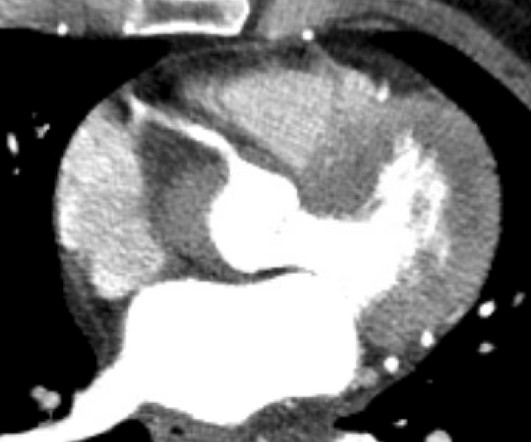
She had this ECG recorded: Obvious massive anterior STEMI She was quickly brought to the critical care area and the cath lab was activated. Here is the ECG at 25 minutes: Terrible LAD STEMI (+) OMI So a CT scan was done which of course showed a normal aorta. This time the Queen of Hearts interpreted: No STEMI or Equivalent.
She presented to the EmergencyDepartment at around 3.5 Final Diagnosis: "STEMI" (of course, as you can see in the ECGs above, this is not true, by definition this was NSTEMI. But the "final diagnosis" commonly just reflects whether the patient was given emergent therapy or not, regardless of the definition of STEMI/NSTEMI).
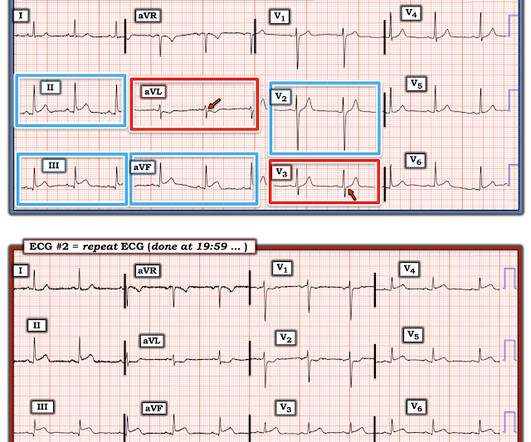
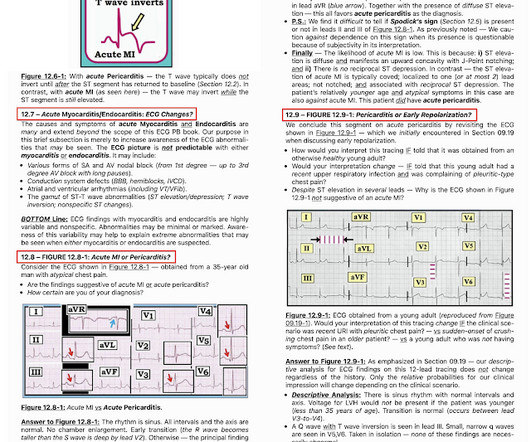
He presented to the emergencydepartment for evaluation. 50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). Lets us consider two different clinical presentations. See Raitt et al.:
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content