This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
3) We do not show the upward concavity measurement technique here. == MY Comment , by K EN G RAUER, MD ( 11/27 /2024 ): == For optimally time-efficient identification of acute OMI in the absence of frank ST elevation — it's essential to get good at recognizing hyperacute T waves. "A A picture is worth 1,000 words".
For instance, there was no protocol for stroke or STEMI. At some point along the way we had protocols for spinal motion restriction, alcohol withdrawal, stroke and STEMI, CPAP, and termination of cardiac arrest resuscitation on scene. The 2024 document is 237 pages including 56 medications. Paramedics didnt do 12-lead ECGs then.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. This was sent to me by an undergraduate name Hans Helseth, who is an EKG tech, but who is an expert OMI ECG reader. He wrote most of it and I (Smith) edited.
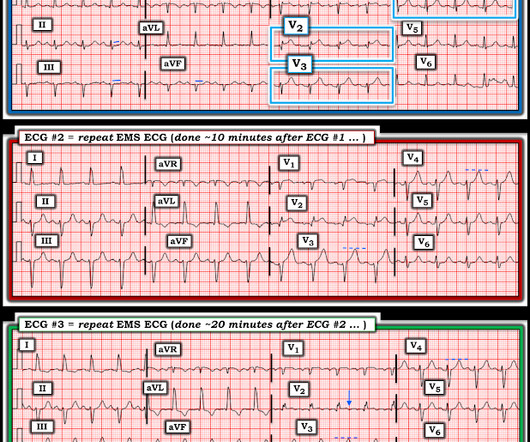
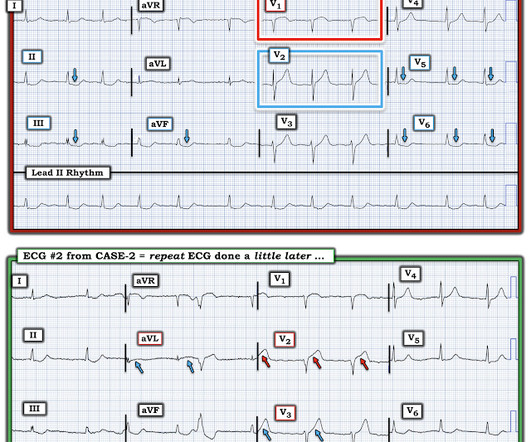
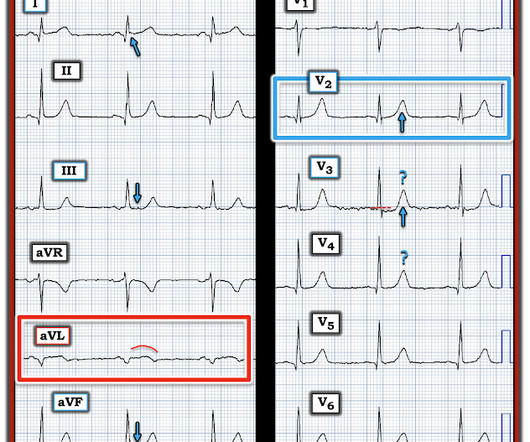
Interpretation : diagnostic of acute anterior OMI with STE less than STEMI criteria in V1-V4, hyperacute T waves in V2-V4, and suspiciously flat isoelectric ST segments in III and aVF suspicious for reciprocal findings. Now it even meets STEMI criteria, and HATWs continue to inflate. So the cath lab was not activated. Ongoing OMI.
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. I would strongly consider the possibility of pure coronary spasm given the history, negative troponins and normal cath in light of the ECG changes seen below in Figure-1 ( See My Comment in the June 5, 2024 post by Dr. Nossen ).
Subtle as a STEMI." (i.e., Here is the bottom line of the article: It is widely believed that hyperacute T-waves are a transitional state preceding ST Elevation 1–4 Thus, it is tempting to postulate that early cases of OMI will eventually evolve to STEMI; yet, our data contradicts that notion. This one is easy for the Queen.
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
If we took this as the gold standard, we would conclude that the computer interpretation was safe and accurate at least accurate enough to not miss STEMI, and that physicians should not be interrupted to interpret it, because there would be no change in patient management. What is the gold standard for ECG interpretation: patient outcome!!!
2024 Aug;84(2):226-227. 2: Human, Take this Patient to the Cath Lab – AI and STEMI Detection Spoon Feed These researchers developed and trained a deep ensemble artificial intelligence (AI) model to classify ECGs as STEMI versus non-STEMI. 2024 Jul 25:S0196-0644(24)00327-5. 2024 Jul 1;154(1):e2023064364.
Obvious infero-postero-lateral STEMI(+)OMI, regardless of context Now let’s put them in order: what was the sequence? With serial ECGs that are ‘STEMI negative’ the physician could have waited for serial troponin levels or referred the patient as “non-STEMI”. 2 Normal ECG #3. What was the outcome and final diagnosis?
Despite anticipation by many that the initial post-resuscitation ECG will show an obvious acute infarction — this expected "STEMI picture" is often not seen. As per My Comment in the above-cited Oct. 15, 2022 post — I like to focus on the ST-T wave appearance in leads V1 and V6 to facilitate recognition of Precordial Swirl.
From April 2-5, the top fire services and EMS industry thought leaders and data analysts gathered at Wave 2024 to share what trends they’re forecasting for both fields and how they’re enacting change within their own organizations through the power of data-driven insights. It’s four days of thought leadership, networking, and learning.
So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
This certainly looks like an anterior STEMI (proximal LAD occlusion), with STE and hyperacute T-waves (HATW) in V2-V6 and I and aVL. How do you explain the anterior STEMI(+)OMI immediately after ROSC evolving into posterior OMI 30 minutes later? This caused a type 2 anterior STEMI.
1: Emergent Cath Lab Activations with “Normal” Computer ECG Interpretations Spoon Feed A significant minority of code STEMI patients have an initial normal computer ECG interpretation. 2024 Mar;31(3):296-300. Originally published at JournalFeed , a site that provides daily or weekly literature updates. Acad Emerg Med. Epub 2023 Sep 17.
Written by Bobby Nicholson What do you think of this “STEMI”? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). With EMS, patient had a GCS of 3 and was saturating 60% on room air. or basilar ischemia.
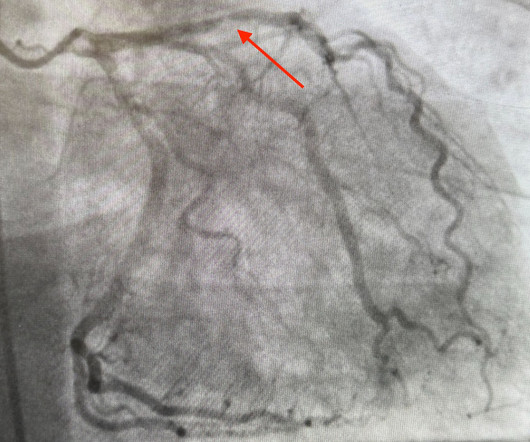
This was a machine read STEMI positive OMI. The meaning of this quote is that at times, something as obvious as the dramatic anterior lead ST elevation that we see in today's tracing is not the result of an acute LAD STEMI. His ECG is shown below. Pretty obvious anterior current of injury. What would you guess is the culprit artery?
So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. The patient was admitted as ‘NSTEMI’ which is supposed to represent a non-occlusive MI, but the underlying pathophysiology is analogous to a transient STEMI. West J Emerg Med 2024). Fortunately the patient did not reocclude while awaiting the angiogram.
Its hard to measure the STE in I exactly with the moving baseline, but there is almost certainly not enough STE to meet STEMI criteria. The ACC recognizes these findings as formal STEMI equivalents (though they do not define how to find them). They are symmetric, fat, convex on both sides, etc.
While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. This case is an example of the steps we can all take in daily practice as the paradigm shifts from STEMI to OMI.
2024 Jan;75:137-142. 2024 Jan;22(1):140-151. 3: New AI-Powered OMI Detector Spoon Feed An artificial intelligence (AI) ECG model outperformed standard STEMI criteria in identifying occlusion myocardial infarction (OMI) confirmed by coronary angiography. It’s time to learn smarter. Am J Emerg Med. doi: 10.1016/j.ajem.2023.10.049.
Discharge ECG showed antero-inferior reperfusion T wave inversion: Had the initial ECG been signed off as “STEMI negative” the patient could have arrested in the waiting room, with a poor cardiac and neurological outcome. A healthy 45-year-old female presented with chest pain, with normal vitals. What do you think? But which one is it?
Cardiac arrest #3: ST depression, Is it STEMI? or is he an ACCESS Trial Candidate? == MY Comment , by K EN G RAUER, MD ( 7/5 /2024 ): == Clinical ECG interpretation is a 2-Step process. The ST depression usually resolves, or is clearly resolving (getting much better). Then assume there is ACS. or is he an ACCESS Trial Candidate?
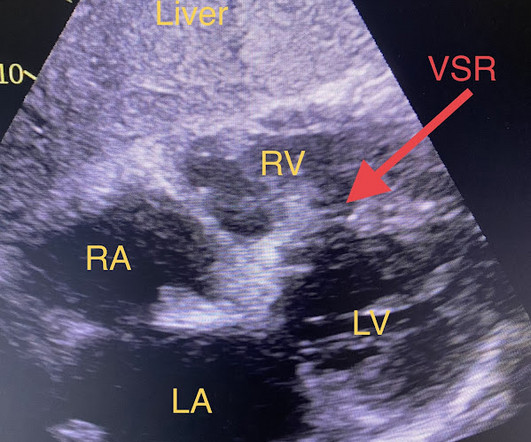
The conventional machine algorithm interpreted this ECG as STEMI. See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI. I've excerpted the Table shown below in Figure-2 from My Comment in that June 17, 2024 post. When EMS found her, she was dyspneic and diaphoretic.
Now it is a full blown STEMI of 3 myocardial territories: inferior, posterior, and lateral But at least it does not call it "Normal." Learning Points: You cannot trust conventional algorithms even to find STEMI(+) OMI, even when they say "normal ECG." At this point — a STEMI was diagnosed, and cardiac cath with PCI was performed.
It has been estimated that in the aggregate, they occur at a rate of about 3 per 1000 patients with acute MI, and most of these events occur in patients with STEMI. It has been estimated that in the aggregate, they occur at a rate of about 3 per 1000 patients with acute MI, and most of these events occur in patients with STEMI.
The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. The paramedic notes called STEMI into question: “EMS disagree with monitor for STEMI callout. Do either, both, or neither have occlusion MI? Vitals were normal.
Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). As far as I can tell, there is only one randomized trial of immediate vs. delayed intervention for transient STEMI. Labs ordered but not yet drawn.
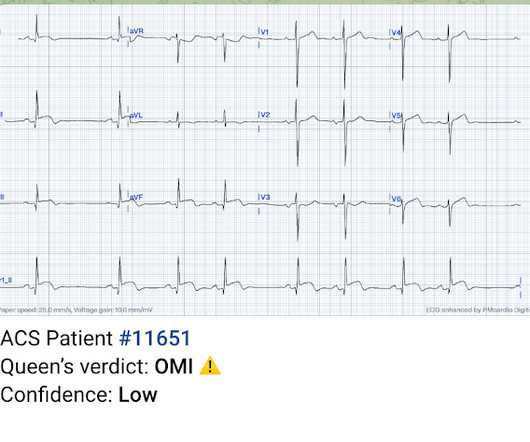
QOH versions 1 and 2 both say Not OMI, with high confidence, without any clinical context, despite the abnormal STE meeting STEMI criteria. The patient did well. == MY Comment , by K EN G RAUER, MD ( 8/4 /2024 ): == I thought today's case by Dr. Meyers is an important one for emergency providers for a number of reasons.
Smith : there is some minimal ST elevation in V2-V6, but does not meet STEMI criteria. Transient STEMI has been studied and many of these patients will re-occlude in the middle of the night. Is it normal STE? The computer thinks so, and the physician thinks that is quite possible. However , there is terminal QRS distortion in lead V3.
This is documented as a STEMI in the clinical notes and in the cath report, but certainly does not meet STEMI criteria and is therefore an NSTEMI by definition. For national registry purposes, this will be incorrectly classified as a STEMI.) Most STEMI have peak cTnI greater than 10.0. Large STEMI are approximately 30-80.
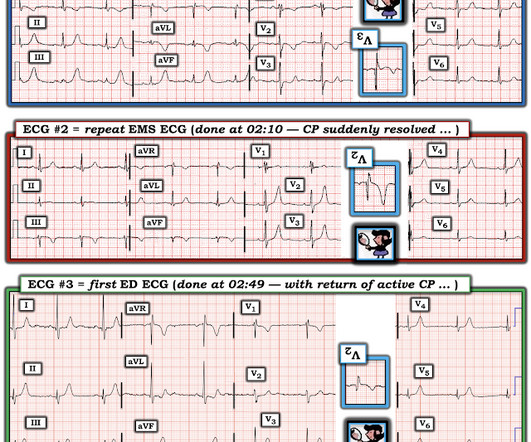
Unfortunately you can see that the conventional Zoll algorithm sees nothing even to suggest AMI, let alone STEMI. Really unusual to me that QOH V1 only has low confidence, but at least its correct. During EMS transport, the pain suddenly resolved.
His EKG with worse pain now shows enough ST elevation to meet STEMI criteria. The EKG was read by the conventional computer algorithm as diagnostic of “ACUTE MI/STEMI”. The patient started receiving medications for “STEMI” (including heparin!!!) Surely, he should be given heparin and taken for an emergent angiogram, right?
The emergency physician asked the advice of Dr. Reiters because of absence of STEMI criteria. But if the pain is persistent, as reported, then the patient must go to the cath lab even if the ECG suggests reperfusion. This will be corrected in Version 2, coming soon. YOU TOO CAN HAVE THE PM Cardio AI BOT!! (THE
Smith comment: No patient over 25 years of age with unexplained chest burning should be discharged without a troponin rule out, no matter how normal the ECG. A diagnosis of "reflux" or "GERD" is never supportable without a troponin rule out. Thus, one considers a test result that varies by 2 or less to be the same result. Heitner et al.
Easy LINK — [link] — My New E CG P odcasts ( 5/28/2024 ): These podcasts are part of the Mayo Clinic Cardiovascular CME Podcasts Series ( "Making Waves" ) — hosted by Dr. Anthony Kashou. 2:25 — Dr. Grauer: The 1st Error : Too many clinicians in 2024 are still stuck in the outdated millimeter-based STEMI Paradigm”.
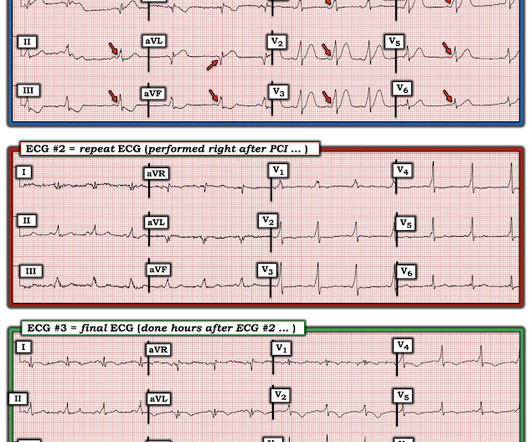
At 2111, the troponin I peaked at 12.252 ng/mL (this is in the range of STEMI patients, quite high). At 1010, the first troponin I (URL 0.034 ng/mL) returned elevated at 0.4 At 1321, a repeat troponin I returned at 0.62 The T waves have deflated significantly and V2 shows the terminal T wave inversion typical to reperfusion.
Another missed OMI by the False STEMI-NonSTEMI Dichotomy Don't miss them!!! Here's what Version 1 QOH thinks: It is diagnostic of acute LAD OMI, with the precordial swirl pattern. Stopped measuring troponins on the day of presentation around 5,000 ng/L as it was still rising." Use the Queen of Hearts and save myocardium and lives!
It definitely does not fulfill STEMI criteria, and I would argue that it would not lead to cath lab activation in most centers. In any case, the ECG is diagnostic of severe ischemia and probably OMI. Smith Modified Sgarbossa Criteria for LBBB and Ventricular Paced Rhythm : 1. Concordant STE of 1 mm in just one lead or 2a.
Later, I found old ECGs: 5 month prior in clinic: V5 and V6 look like OMI 9 months prior in clinic with no chest symptoms: V5 and V6 look like OMI 1 year prior in the ED with chest pain: V5 and V6 sure look like a STEMI For this ECG and chest pain in the ED, the Cath lab activated. But the angiogram was clean. There was no OMI.
The ECG was read as "No STEMI" and the patient was treated like an average chest pain patient (despite the fact that a chest pain patient with active pain and active subendocardial ischemia is very high risk). The Queen of Hearts AI app will hopefully be FDA approved in Q1 of 2024. He was diagnosed as NSTEMI.
This ECG is highly concerning for LAD occlusion despite it not showing a STEMI criteria. You can find the variables used to calculate the value on MD calc here: [link] Utilizing Dr. Smith’s Subtle Anterior STEMI Calculator (4-Variable), the value is greater than 18.2 Chest Pain – Benign Early Repol or OMI?
The paramedic called the EM physician ahead of arrival and discussed the case and ECGs, and both agreed upon activating "Code STEMI" (even though of course it is not STEMI by definition), so that the acute LAD occlusion could be treated as fast as possible. So the cath lab was activated. Long term outcome is unavailable.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content