This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Welcome to the first episode of the Broomedocs podcast for 2025. Justin and I are back for more nerdy goodness to make you smarter in the Resus room, or at a pub trivia night more likley… wether it is about salt correction, dissection or infection we can help you out! Listen in and learn! Dimer is useful in the low risk group.
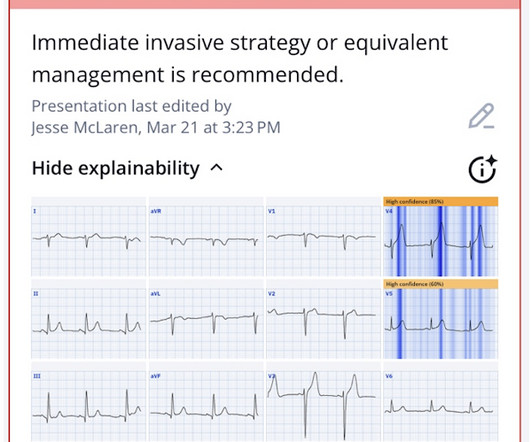
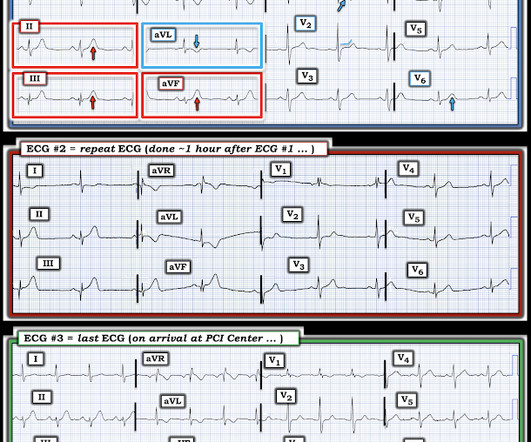
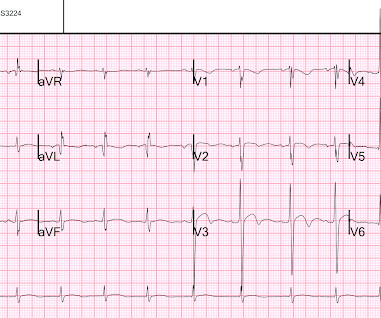
But there are also hyperacute T waves (HATW) in V4-5, which exclude early repolarization and pericarditis, leaving only LAD occlusion for this patient presenting with classic symptoms of ACS. What do you think? What do you think? Theres normal sinus rhythm with normal conduction, right axis and delayed R wave, and normal voltages.
T-wave inversions in the acute phase of ACS are usually a welcome finding, indicating reperfusion. In a patient with ACS symptoms disappearing TWI should be considered re-occlusion of the infarct related artery. If TWI disappears or reverses, always consider re- occlusion ( pseudonormalization )! Clin Cardiol [Internet].
Discussion: This case highlights many important points worthy of discussion, mainly because it represents very routine care for ACS but there are so many ways we could improve outcomes with tools we already have! Troponin was rising when last checked, 8928 ng/L. A recent meta-analysis by Stone et al.
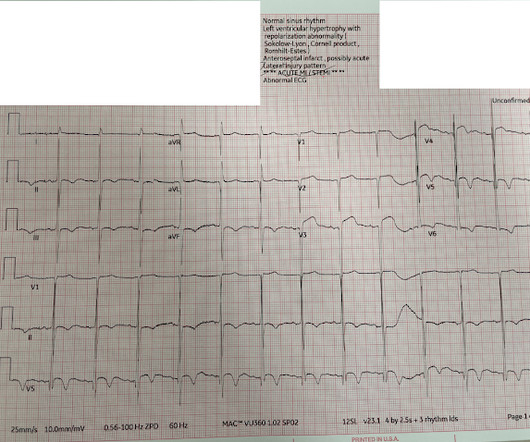
So the final diagnosis is STEMI, and there is no question or feedback about whether the acute coronary occlusion could have been identified sooner. If I were the patient, I would want intervention to be 2 hours earlier, wouldn't you? What would you want? Is the disease the ST segment? or is the disease acute coronary occlusion?
Before your trauma registry software can be updated with the annual trauma standards, ESO must receive the foundational data standards from the American College of Surgeons (ACS) first. The ACS provides the National Trauma Data Standard 2025 Data Dictionary.
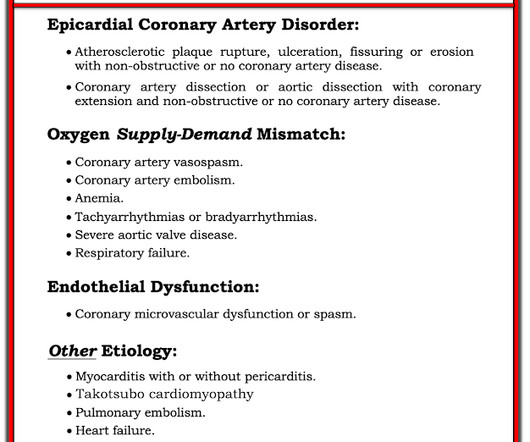
Coronary microvascular dysfunction Coronary dissection Read more about MINOCA and its etiologies here: [link] == MY Comment , by K EN G RAUER, MD ( 4/12 /2025 ): == Today's case brings up several important points regarding the entity known as, "MINOCA" ( = MI with N on- O bstructive C oronary A rteries ). Embolism with lysis.
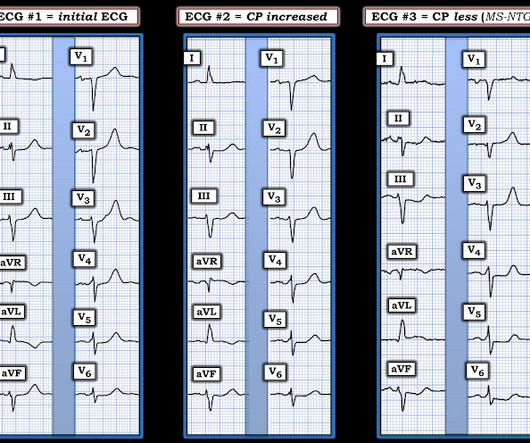
Hyperacute T-waves frequently NEVER progress to diagnostic ST Elevation Patients with ACS and pain refractory to anti-ischemic therapy should be sent emergently for catheterization, regardless of the ECG. It is also possible for hyperacute T waves to remain somewhat stable during either a sustained period of occlusion or partial reperfusion.
Negative trops and negative angiogram does not rule out coronary ischemia or ACS. It is a judgment call retrospectively, but to assume there is no ACS at presentation is very risky, especially in a patient with previously diagnosed severe CAD and poor LV function. It must be diagnosed with IVUS or Optical Coherence Tomography.
2025 Feb 20;188(4):1119-1136.e23. 2025 Feb 20;188(4):1119-1136.e23. Credits & Suggested Citation Episode written by Avi Cooper Show notes written by Avi Cooper and Giancarlo Buonomo Audio edited by Clair Morgan of nodderly.com Cooper AZ, Abrams HR, Breu AC, Buonomo G. April 23rd, 2025. Zhong L et Al. Zhong L et Al.
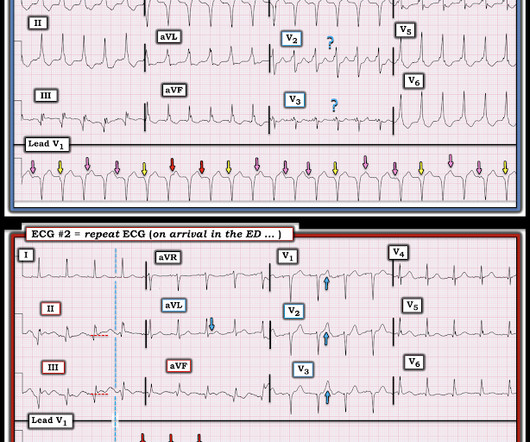
He had several older ECGs on file, here are two examples: 6 days prior: 2 months prior: In the context of ACS symptoms, and when able to compare the new vs. old ECG, the top ECG is DIAGNOSTIC of OMI until proven otherwise. In the absence of old ECGs, one must record serial ECGs every 15 minutes.
When the Queen has some suspicion of OMI, she asks if the patient has ACS Symptoms. The emergency physician does cautiously (correctly) note that the ECG meets STEMI criteria in V3 and V4, but goes on to document absence of ACS symptoms. When I reviewed the chart, I learned that the patient had presented with syncope.
After ruling out for ACS, the patient underwent angiography where he was found to have severe stable disease, which was already known. NOTE: Although this case study is from 1995 the misdiagnosis of wide tachycardias "because the patient is stable" remains all-too-common in 2025.
In ACS, chest pain is the warning sign of ongoing ischemia. Other trials have found a benefit to revascularizing non-culprit lesions when a patient presents with ACS, the largest of which was COMPLETE , and more recently MULTISTARS AMI. Smith : it is highly suspicious for inferior OMI, but not 100% diagnostic. in absolute terms!
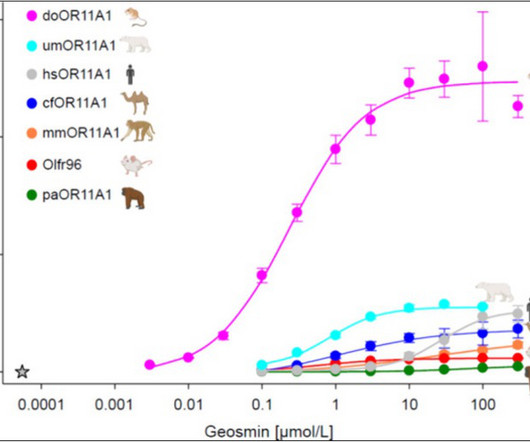
The word argillaceous means “clay-like” and they felt this didnt reflect the broad range of materials which can be associated with this earthy smell, including rocks containing silica or iron oxide. They preferred “petrichor,” which literally means “essence of stone.” But, there may be reason to. for new episodes.
Summary : it is hard to say whether this ST Elevation was initiated by 1) something which led to pulmonary edema, then hypoxia, then supply-demand mismatch, or 2) whether ACS with OMI combined with some other pre-existing condition led to a decrease in LV function and pulmonary edema. We certainly know that there is hypoxia.
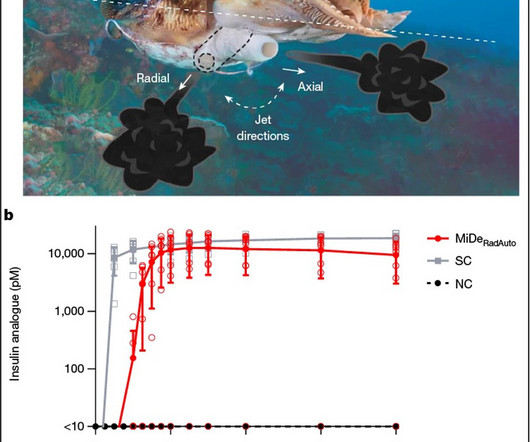
Why don’t we administer insulin orally? In inpatient medicine, a phrase one often hears is “transition to PO.” ” Medications that start out as injections or infusions antibiotics, steroids, anticoagulants are switched to an oral equivalent as soon as possible. What is it about insulin that makes an oral route untenable ?
Credits & Suggested Citation Episode written by Avi Cooper Show notes written by Avi Cooper and Giancarlo Buonomo Audio edited by Clair Morgan of nodderly.com Cooper AZ, Abrams HR, Breu AC, Buonomo G, The Grapes of Pseudomonas’ Wrath. February 12th, 2025. In this episode, we’ll be exploring a more benign side of PA.
Credits & Suggested Citation Episode written by Giancarlo Buonomo Show notes written by Giancarlo Buonomo Audio edited by Clair Morgan of nodderly.com Buonomo G, Abrams HR, Breu AC, Abrams HR, Cooper AZ. January 22nd, 2025. Diabetes is not, in and of itself, a risk factor for all types of Pseudomonas infections. for new episodes.
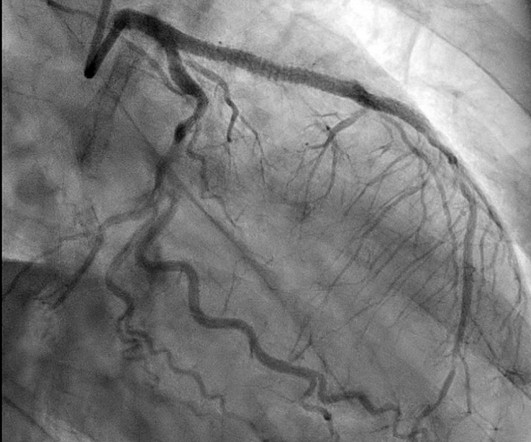
Patients with suspected ACS should be evaluated with echocardiography. It will probably show an occlusion of the LAD, and it might be difficult to know how long the occlusion has been there and how viable the myocardium is, but it needs to be opened. Let us have a look at the limb lead ST-T changes. Is this ST elevation ischemic in nature?
Sea AC, Lensing S, Rompalo A, et al. Sexual Transmitted Infections in Children ? Dr. Jackson, are you gonna have us talk to teens about sex again? Stigma has played a significant role in care for marginalized groups, leading to many health disparities. Therefore, CDC does not recommend risk-factor-based screening.
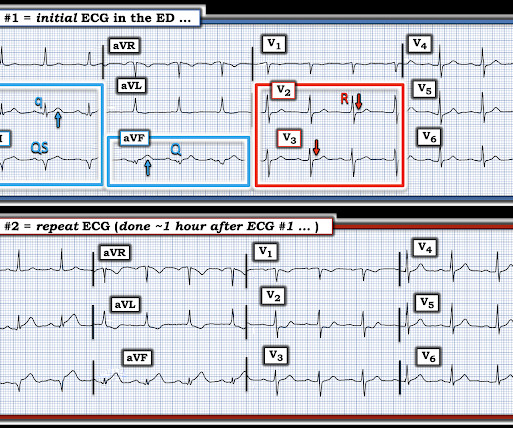
Serial ECGs demonstrated dynamic changes diagnostic of ACS (transient STEMI) 4. Wehrens XH, Doevendans PA, Ophuis TJ, Wellens HJ. A comparison of electrocardiographic changes during reperfusion of acute myocardial infarction by thrombolysis or percutaneous transluminal coronary angioplasty. Am Heart J 2000;139(3):4306. Learning Points 1.
Whenever I see PVCs with the morphology and axis seen in todays case I always look for signs of AC ( Arrhythmogenic Cardiomyopathy ). See this case for an in-depth discussion of AC and an example of VT and ECG changes associated with this disorder. Arrhythmogenic cardiomyopathy often manifests with PVCs from the RV.
Does this patient have ACS Symptoms? He had no symptoms when seated, but felt lightheaded when standing and walking. He played a round of golf a week prior and felt an episode of chest pain during the round, which spontaneously resolved. On presentation, he reported no chest pain or shortness of breath. See Example case at bottom.
After completing the ACS algorithm with amiodarone and lidocaine, there are diminishing returns on further treatments. In lab, patients are monitored on continuous abbreviated ECG with 5 electrodes. During ballooning, we often see immediate hyperacute T waves. The patient's ECG at the beginning of the case is shown below. SanzRuiz, R.,
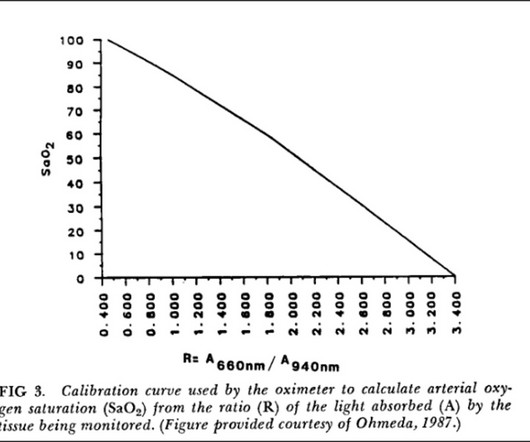
Credits & Suggested Citation Episode written by Tony Breu Show notes written by Tony Breu and Giancarlo Buonomo Audio edited by Clair Morgan of nodderly.com Breu AC, Abrams HR, Cooper AZ, Buonomo G, Pulse Check: Methemoglobin. March 12th, 2025. Listen to the episode ! hours), Non-Physician Attendance (0.5 for new episodes.
Hesseling AC, et al. The post Bubble Wrap PLUS – January 2025 appeared first on Don't Forget the Bubbles. This comprehensive list is developed from 34 journals, including major and subspecialty paediatric journals. During the first days of the new year, many people make solemn resolutions. Mohammed Abdul Wajid L, et al.
The patient denies any current symptoms but states that he just wants to get checked out. He has no chronic medical conditions, does not take any medications, and does not use any drugs or alcohol. Vital signs are within normal limits, with BP 110/70 mmHg, HR 60 bpm, RR 18 breaths/min, O2 saturation 98% on RA, T 37 C.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content