This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
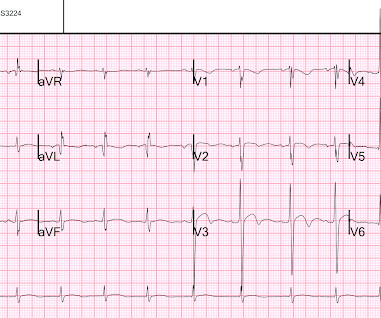
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. What do you think?
If we took this as the gold standard, we would conclude that the computer interpretation was safe and accurate at least accurate enough to not miss STEMI, and that physicians should not be interrupted to interpret it, because there would be no change in patient management. The latest is Langlois-Carbonneau et al.
Save the date for Wave 2025 featuring ESO Training Academy! Taking place from April 22-25, 2025, in Austin, TX, Wave featuring ESO Training Academy is a four-day conference dedicated to the data-driven insights and technological advancements transforming the EMS, fire, and hospital industries.
Save the date for Wave 2025! Taking place from April 22-25, 2025, in Austin, TX, Wave is a four-day conference dedicated to the data-driven insights and technological advancements transforming the EMS, fire, and hospital industries. Supporting and advocating for mental health Mental health calls are increasing.
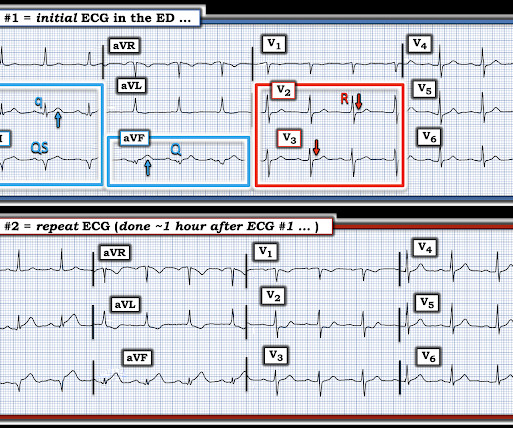
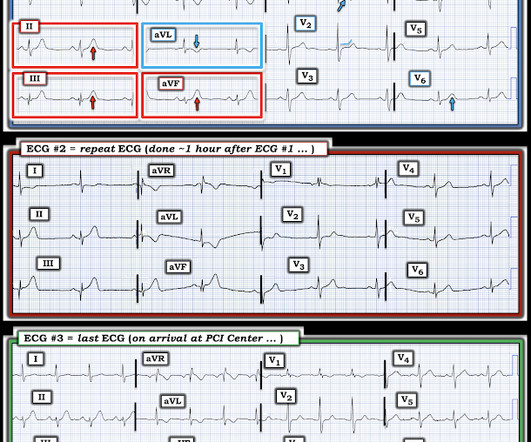
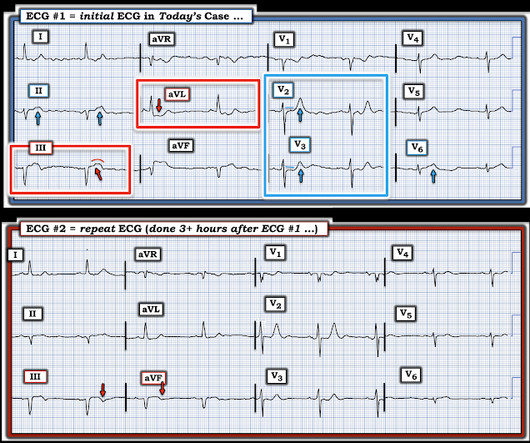
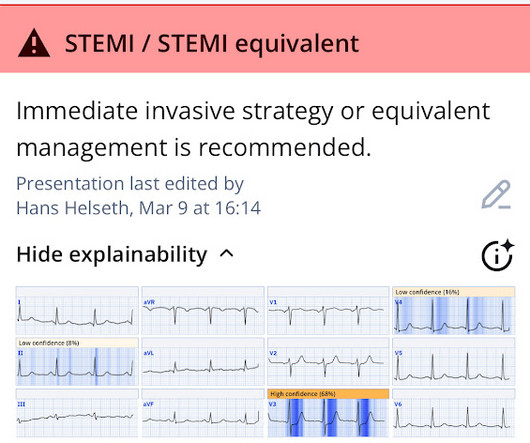
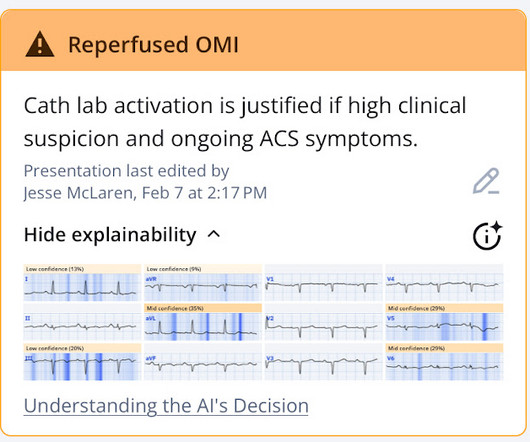
Here is the PMcardio Queen of Hearts interpretation of the ECG: STEMI equivalent detected. Inferior and posterior OMI without STEMI criteria. About an hour later another ECG was obtained: Barely meets STEMI criteria in inferior leads, but obvious inferior and posterior OMI. The cath lab was now activated for STEMI.
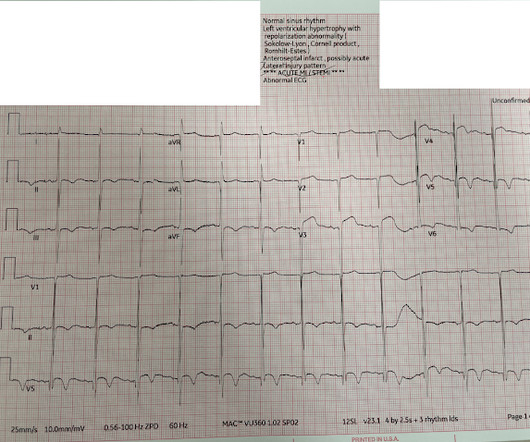
Even before we have clinical context, this ECG simply does not appear concerning for OMI, notwithstanding the machine's interpretation ** ** ACUTE MI / STEMI ** **. But in the world of STEMI, this is a challenging ECG to most. There were 80 positives by STEMI criteria, 88 by device algorithm, and 77 by AI software.
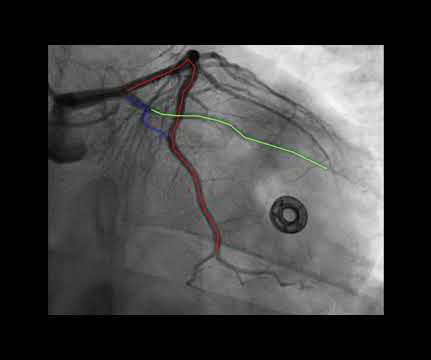
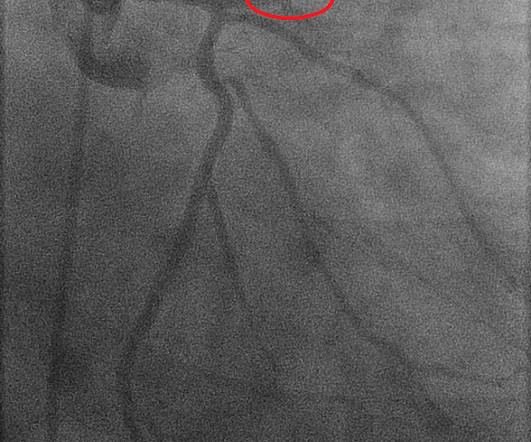
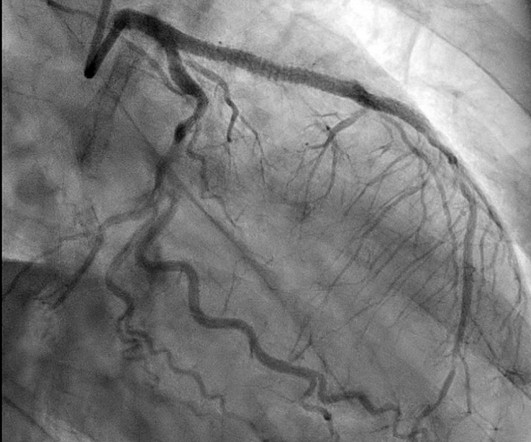
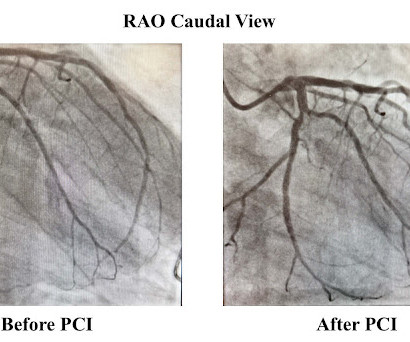
Here is the Queen of Hearts interpretation: Here is the cardiologist's impression: "EKG does not show a STEMI." Here is the cath report (TIMI-2 flow in the circumflex -- stented): Learning Point: Just because the cardiologist says it is "not a STEMI" and "wants to teach you about the ECG", it does not mean you should back down.
The emergency medicine physician documented, "His initial EKG is riddled with artifact and difficult to interpret but does not look like a STEMI." The ECG remains positive for STEMI by GE. The absolute degree of ST elevation (although enough to meet STEMI criteria), was still relatively small.
Im changed. == MY Comment , by K EN G RAUER, MD ( 1/16 /2025 ): == It's not often that we see a clinical entity for which it seems that the patient "read the textbook" before the ECG was recorded. He wrote: OMI it was. Large diagonal. Now opened. Dr. Smithyoull change MI care, if you havent already.
This ECG pattern is my favorite example of how the STEMI criteria are fundamentally flawed. We have a series of 20 TIMI-0 LAD Occlusions that do meet STEMI criteria. However, many patients with de Winter ECG pattern have TIMI 0 at angiography and the ECG pattern does not necessarily progress to STEMI. 17 have HATW. Under Review.
His first EKG is shown below, with a lead II rhythm strip: EKG 1, 1645 A provisder who is looking for STEMI would not see much in this EKG. It is possible that the T waves in this EKG are of an intermediate morphology between full-blown STEMI and inferior reperfusion. This is the classic morphology of hyperacute T waves.
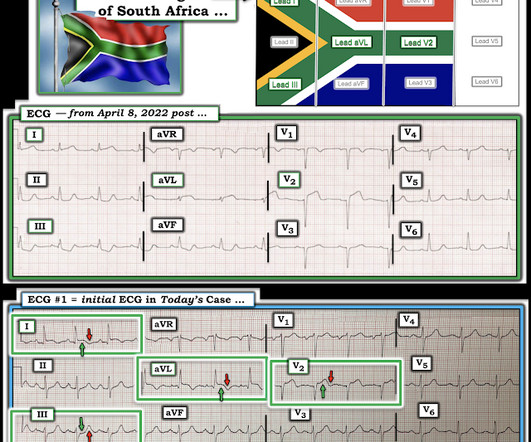
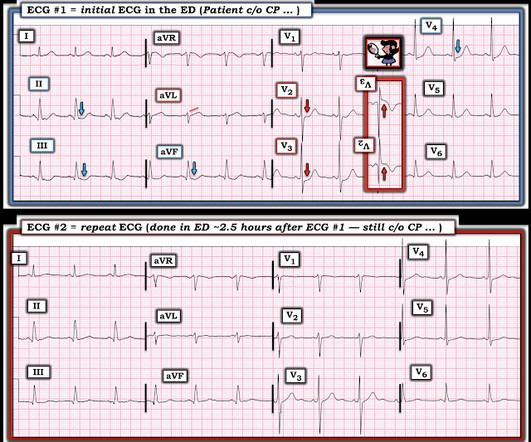
He has a history of coronary artery disease and a STEMI two years prior that was treated with primary PCI. At the time of this initial ED ECG, his symptoms were improving ECG #1 on admission to the ED The patient was not seen quickly in the ED as it was a busy shift and the ECG did not meet STEMI criteria. The below ECG was recorded.
They recorded this ECG: Obvious inferior STEMI/OMI What else? I suspect this statement is still true 2 years later, in 2025. The EMS ECGs: As per Dr. Smith the diagnosis of acute inferior STEMI is obvious from the history of new, severe CP in a patient with the initial EMS ECG that I show below ( TOP tracing in Figure-1 ).
Note: the 2022 ACC Expert consensus Chest pain guidelines state that "posterior STEMI-Equivalent" is a sign of acute coronary occlusion. 2/3 of STEMI have a peak 4th generation troponin I greater than 10.0 Comment: The first ECG is diagnostic of OMI that does not meet STEMI criteria. NSTEMI-OMI").
Limitations of registry data: This patient presented with STEMI (-) OMI and developed STEMI the following day. But the time that elapsed from first STEMI (+) ECG to balloon was 57 minutes, and THIS is what will be recorded for reporting to the National Cardiovascular Data Registry for purposes of quality improvement.
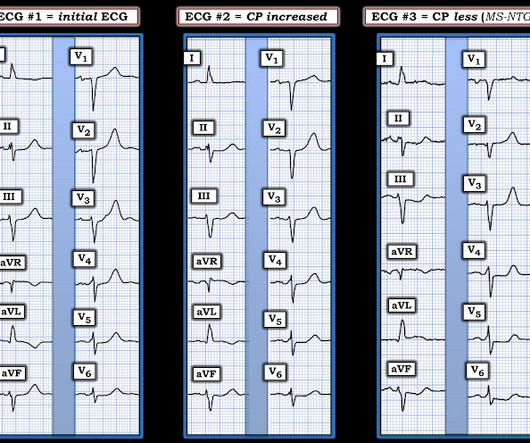
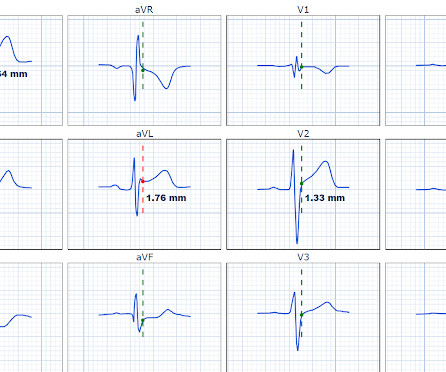
STEMI criteria are only 43% sensitive for OMI. Regarding the ECG, this case shows inferior ST elevation with reciprocal depression in aVL that does not quite meet STEMI criteria, ST depression maximal in V2-V3 (>97% specific for posterior MI), and an increasingly anterior R wave progression indicating posterior wall infarction.
Learning points: 40% of LAD OMI with TIMI-0 flow do NOT meet STEMI criteria (manuscript under consideration at Eur Ht. 20/53 did not meet STEMI criteria, but all showed OMI diagnosed by both Smith and the Queen of Hearts. Another left ventricle sacrificed at the alter of ST elevation. J Cardiovascular Interventions.--20/53
Unfortunately, the ECG was interpreted as no significant change from prior , "no STEMI"!! Approximately 5 minutes after ROSC, this ECG was obtained (about 45 minutes after arrival): Obvious anterolateral OMI, and STEMI criteria positive for those who care or need it. He was sent back to the waiting room, where he suffered a VF arrest.
At 1210, the case was discussed with a cardiologist at a PCI capable facility, who accepted the patient for transfer, noting the ST depression in anterior leads as consistent with ischemia but not a STEMI. 5 years later ( now in 2025 ) the problem remains. 5 years later ( now in 2025 ) the problem remains.
Supply-demand mismatch can cause ST Elevation (Type 2 STEMI). Also see these posts of Type II STEMI. An EKG from a year prior was available for comparison: The ED physician noted Initial EKG here read by the computer as a STEMI, however, there is a very poor baseline and a lot of artifact. See reference and discussion below.
Peaked T waves: Hyperacute (STEMI) vs. Early Repolarizaton vs. Hyperkalemia Recognize subtle findings of hyperK and, if present, treat with Calcium immediately! HyperKalemia with Cardiac Arrest. References 1. Lindner et al. Acute hyperkalemia in the emergency department: a summary from a Kidney Disease: Improving Global Outcomes conference.
This was interpreted as "inferior STEMI" and the cath lab was activated. Discharge diagnosis was Non-STEMI. The STEMI/NSTEMI dichotomy can make it difficult to identify the culprit lesion, which can be spontaneously reperfused at the time of the angiogram 3. The patient had no further episodes of chest pain.
The ECG meets STEMI criteria objectively. Abdominal Pain in a middle-aged patient True Positive ST elevation in aVL vs. False Positive ST elevation in aVL == MY Comment, by K EN G RAUER, MD ( 2/10/2025 ): == I find cases like today's challenging. PM Cardio QOH says No signs of OMI. AMI was ruled out.
It is correct that he did not have chest pain, but we must remember that fully 1/3 of full blown STEMI do not present with chest pain. This is extremely elevated for a type 2 MI and totally consistent with STEMI. As per Dr. Smith the Troponin peak of 16,000 is much more suggestive of a STEMI than of a Type II MI.
The paramedics diagnosis was "Possible Anterolateral STEMI." More proof that a huge STEMI may have normal or near normal initial troponin. Taken together, these findings suggest an ongoing extensive antero-lateral STEMI. I don't know what the device algorithm interpretation stated. The final angiographic result is very good.
A 12-lead was recorded, showing "STEMI," but is unavailable. Moreover, if you know that catastrophic intracranial hemorrhage can result in an ECG that mimics STEMI, then you know that this patient probably has a severe intracranial hemorrhage. She was BVM ventilated and suctioned. Shortly thereafter, pulses were lost.
He has never been poisoned by the STEMI/NSTEMI paradigm because he has never been to medical school. The Queen of Hearts recognizes this as OMI ("STEMI/STEMI Equivalent"). He just graduated from college. He has no medical training, but he has read this blog for years. He is an ECG tech who hopes to go to medical school.
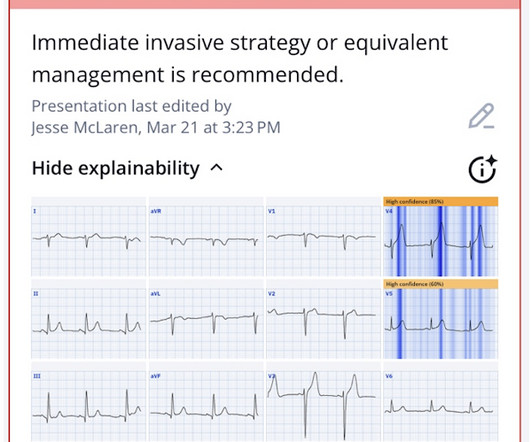
Here is the Queen of Hearts interpretation, appropriately reading STEMI equivalent, highlighting anterior and lateral leads with explainability, and even detecting reduced LVEF. The Cardiologist stated that the ECG did not show signs of STEMI, but rather NSTEMI, recommended serial ECGs and troponins, and cancelled the activation request.
Here is the prehospital ECG, recorded in the presence of pain: Hyperacute anterolateral STEMI The medics had activated the cath lab and the patient went for angiogram and had a 95% stenotic LAD with TIMI-3 flow. So even a massive STEMI, if it reperfused quickly, can result in a relatvely low troponin (in contrast to the next case!)
50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). link] == MY Comment , by K EN G RAUER, MD ( 1/14 /2025 ): == I found today's case highly insightful with regard to many aspects. See Raitt et al.:
Acute chest pain, right bundle branch block, no STEMI criteria, and negative initial troponin. check out the downsloping STE in this one A man in his 80s with chest pain What, besides large anterior STEMI, is so ominous about this ECG? These are often VERY difficult to recognized.
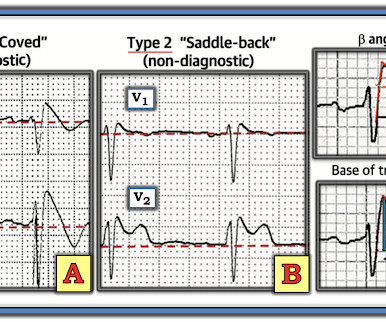
How well does the computer interpretation perform? -- in this case, the computer diagnosed STEMI but the patient had Fever with Brugada -- A young F is hyperthermic, delirious, and dry: Fever-induced Brugada? Diphenhydramine toxicity?
link] == MY Comment , by K EN G RAUER, MD ( 1/20 /2025 ): == If you Google, Broken Heart Syndrome you will immediately see reference to many pages of Patient Education news briefs and informationals, in which the questions addressed are, Can You Really Die of a Broken Heart? & Dawson, D. Circulation , 145 (13), 10021019.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content