This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Davidson JS, Brown DJ, Barnes SN, et al. West S, Andrews J, Bebbington A, et al. Symons S, Rowsell M, Bhowal B, et al. J Pediatr Orthop. 2018;Volume 00(00):DOI:10.1097/BPO.0000000000001169. 0000000000001169. Simple treatment for torus fractures of the distal radius. J Bone Joint Surg Br. 2001;83:1173-5. Pediatr Emerg Care.
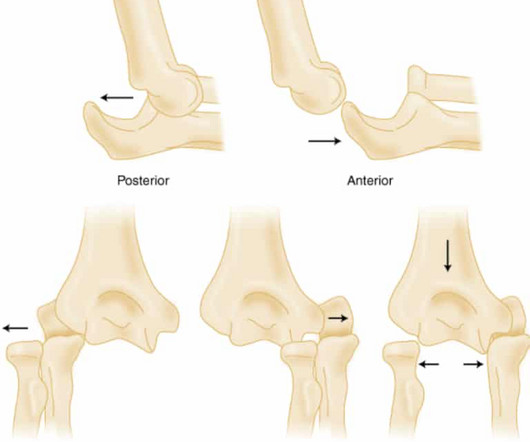
PMID: 32644703 Robinson PM, Griffiths E, Watts AC. PMID: 27227986 Glover NM, Black AC, Murphy PB. Commentary on an article by Marc Schnetzke, MD, et al.: “Determination of Elbow Laxity in a Sequential Soft-Tissue Injury Model. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. Simple elbow dislocation. 2023 Nov 5.
Studies such as those by Moise et al 14 and Ellis et al 39 have shown that the relative risk of developing an acute myocardial infarction in the territory supplied by an artery with a 70%. years, with the interval as long as 12 or 18 years in some studies. Nor was there a challenge to look for coronary spasm.
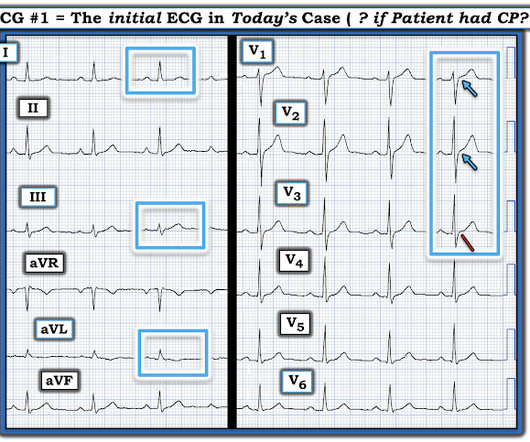
You turn to the attending and ask, “do you really think this could be acute coronary syndrome (ACS)?” ACS is usually amongst this differential, as cardiovascular disease is a leading cause of morbidity and mortality in this population. Reference: Wang et al. The utility of troponin testing to diagnose or exclude ACS. *
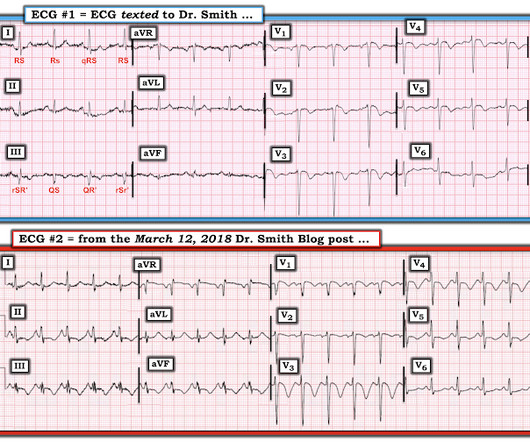
Although the attending crews did not consider the ECG pathognomonic for occlusive thrombosis, they nonetheless considered the patient high-risk for ACS and implored him to reconsider. The attending crews were concerned for an ACS-equivalent of LAD occlusion and initiated a prehospital STEMI activation to the closest PCI center.
Date: September 8th, 2021 Reference: Desch et al. Date: September 8th, 2021 Reference: Desch et al. Defibrillation is the treatment of choice in these cases but does not often result in sustained ROSC ( Kudenchuk et al 2006). Acute coronary syndrome (ACS) is responsible for the majority (60%) of all OHCAs in patients.
As per my review of this subject ( Check out My Comment at the bottom of the page in the November 16, 2023 post in Dr. Smith's ECG Blog ) — the 3 most common Causes of ACS ( A cute C oronary S yndrome ) with a "negative" cath are: i ) Myocarditis; ii ) Takotsubo cardiomyopathy; and , iii ) MINOCA.
Date: June 30th, 2022 Reference: McGinnis et al. Date: June 30th, 2022 Reference: McGinnis et al. If we thought about ACS, we brought them in. Reference: McGinnis et al. Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? AEM June 2022. AEM June 2022. AEM June 2022.
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). ACS and hyperkalemia both have lethal downstream consequences, so it is imperative for the clinician to acclimate to the presentation, or developing, features of each. link] [1] Zachary et al. 2] Costanzo, L.
Reference: Brichko et al. Reference: Brichko et al. Reference: Brichko et al. Chris Bond is an emergency medicine physician and assistant Professor at the University of Calgary. He is also an avid FOAM supporter/producer through various online outlets including TheSGEM. AEM Feb 2021. AEM Feb 2021.
Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. Lindahl et al. From Gue at al. Most studies examine undifferentiated ACS cohorts, with only a handful providing separate data.
VS abnormalities can drive this as well Strongly consider reversal of AC (this will typically come after control) Stopping the Bleeding PPE: these things bleed like stink. EMRAP HD: Epistaxis Posterior Pack References Cassisi NJ et al. PMID: 5569677 Zeyyan E et al. PMID: 20938948 Loftus BC et al.
Date: May 24th, 2022 Reference: Broder et al. Date: May 24th, 2022 Reference: Broder et al. Reference: Broder et al. Guidelines for Reasonable and Appropriate Care in the Emergency Department (GRACE) 2: Low-Risk, Recurrent Abdominal Pain in the Emergency Department.
100% seems too good to be true Morello et al., Clin Exp Allergy. 2024 Oct 9. doi: 10.1111/cea.14565. Epub ahead of print. PMID: 39383344 Profundus Trial – Can we actually exclude acute aortic syndromes with this protocol? Diagnosis of acute aortic syndromes with ultrasound and D-dimer: the PROFUNDUS study. Emerg Med J. Epub 2018 Oct 25.
doi:10.1093/tropej/fmz071 Expert Panel on Pediatric Imaging, Trofimova A, Milla SS, et al. 2019-0134 Hirtz D, Ashwal S, Berg A, et al. Riviello JJ Jr, Ashwal S, Hirtz D, et al; American Academy of Neurology Subcommittee; Practice Committee of the Child Neurology Society. J Trop Pediatr. 2020;66(3):299-314. J Am Coll Radiol.
Thus, these troponins are very concerning for ACS, and subsequent ones will probably be diagnostic of acute MI. Heitner et al. For this test it is VERY low (very good) at 4% at the 99th percentile -- 26 ng/L, but it will not be so good at a level of 9 ng/L. The troponin is trapped in the myocardium that is not being perfused.
Antonaci L, et al. Tritos NA, et al. Levi M, et al. Fishbein MH, et al. Cetinkaya PG, et al. Niu T, et al. Verkuijl SJ, et al. Varni JW, et al. Dias FC, et al. Peter C, et al. Ahlberg R, et al. Shir A, et al. Kuypers KLAM, et al. Hegeman EM, et al.
In our opinion it should not be given in ACS unless you are committed to the cath lab. Learning Point: Any NSTEMI patient with active ongoing ACS symptoms refractory to medical management is supposed to go to the cath lab within 2 hours if available, per all guidelines in world, regardless of ECG findings. Am J Emerg Med.
Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1] Amsterdam et al. Alencar et al. Lupu et al. Herman, Meyers, Smith et al. But only 6.4% link] References 1.
Growdon ME, Jing B, Morris EJ, Deardorff WJ, Boscardin WJ, Byers AL, Boockvar KS, Steinman MA. Credits & Suggested Citation Episode written by Tony Breu Show notes written by Giancarlo Buonomo and Tony Breu Audio edited by Clair Morgan of nodderly.com Breu AC, Abrams HR, Cooper AZ, Buonomo G. J Am Geriatr Soc. October 2nd, 2024.
The original term " benign early repolarization" has fallen out of favor since the seminal paper by Haïssaguerre et al. As a result, even before looking at this patient's initial ECG — he falls into a high -prevalence likelihood group for ACS ( for an A cute C oronary S yndrome ). per 100,000 to 11 per 100,000 [Rosso].
Read More First10EM: Imaging for Renal Colic SGEM : SGEM XTRA: COME TOGETHER, RIGHT NOW – OVER RENAL COLIC References Chang, Helena, et al. Moore CL, Carpenter CR, Heilbrun ME, et al. Smith-Bindman R, Aubin C, Bailitz J, et al. PMID: 25229916 DOI: 10.1056/NEJMoa1404446 Westphalen AC, Hsia RY, Maselli JH, Wang R, Gonzales R.
But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. Dialysis patients have a high rate of ACS without chest pain and high rate of delayed diagnosis and delayed reperfusion 2.
Follow up with the dentist in the morning Reinsert the tooth and avoid solid food Reinsert the tooth and stabilize it with a bridge Remove the tooth and repair the gingival laceration Remove the tooth and wrap it in saline-soaked gauze FOR THE RIGHT ANSWER CLICK ON THE ROSH REVIEW LOGO BELOW References Day PF, Flores MT, O’Connell AC, et al.
The cath report showed: Significant stenosis with subtotal occlusion (99%) in the prox to mid Lcx, culprit of ACS, TIMI flow 1. Available from: [link] If you are wondering about the Barcelona rule, then you should read the above paper by Khawaja et al. Cardiac catheterization occurred around 1pm (18 hours after arrival). 2021;23:187.
Anecdotally, had there been symptoms unequivocally consistent with ACS then one could justifiably make the case for a potential D1 occlusion. 4] Baranchuk, A, et al. Given such findings, serial ECG’s are prudent to consider, and carry significant impact moving forward, which has been demonstrated in previous posts. 2] Surawicz, B.
Many conditions outside of acute coronary syndrome (ACS) mimic ST-elevation myocardial infarction (STEMI), but only a handful of cases have reported ST-elevations (STE) in the setting of pancreatic inflammation where underlying ACS was excluded. 2 Proposed hypothesis as described by Hsu et al., Yu ES, Lange JJ, Broor A, et al.
The NIHSS cutoff that predicts outcomes is 4 points higher in AC compared with PC infarctions. References: Gaillard F, Glick Y, Tatco V, et al. 61.4.496 Navi BB, Kamel H, Shah MP, et al. Goldmakher GV, Camargo EC, Furie KL, Singhal AB, Roccatagliata L, Halpern EF, et al. link] Burns JD, Rindler RS, Carr C, et al.
Because there was proven thrombus (ACS) but the troponin never went above the 99% reference range (and therefore cannot be called MI -- definition of MI requires rise and/or fall of troponin with at least one value above the 99% reference range), this is UNSTABLE ANGINA with ST Elevation.
Some providers were worried about ACS because of this ECG. My answer alleviated their concern for ACS and no further workup was done for ACS. Kosuge et al. showed that , when T-waves are inverted in precordial leads, if they are also inverted in lead III and V1, then pulmonary embolism is far more likely than ACS.
Smith: If this is ACS (a big if), t his is just the time when one should NOT use "upstream" dual anti-platelet therapy ("upstream" means in the ED before angiography). History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. Knotts et al.
There were zero patients in this study with a "normal" ECG who had any kind of ACS! Deutch et al. This defies all previous data on acute MI which would show that even undetectable troponins do not have a 100% negative predictive value. So this study is actually worthless. West J Emerg Med 2024).
” As a result, Jansen et al. ” As a result, Jansen et al. Despite initial enthusiasm for widespread use, there are minimal data suggesting significant mortality benefit. undertook a pragmatic RCT to investigate the use of REBOA in trauma. . undertook a pragmatic RCT to investigate the use of REBOA in trauma. 2023 JAMA.
Type 1 is the acute deterioration in kidney function seen in cardiogenic shock from ACS. Type 1 is the acute deterioration in kidney function seen in cardiogenic shock from ACS. To start with there are apparently 5 types of cardiorenal syndrome. I’ll let that sink in. You all thought there was one didn’t you? Nijst, P. &
link] Li Z, Krippendorff BF, Sharma S, Walz AC, Lavé T, Shah DK. Bush SP, Ruha AM, Seifert SA, et al. link] Kanaan NC, Ray J, Stewart M, et al. [link] Full prescribing information. Crotalidae polyvalent immune fab (ovine). Published online January 2018. Accessed August 17, 2023. 2016;8(1):113-119. Published online November 2020.
SCAD isn’t rare, especially in women Historically SCAD had been identified in 22% of ACS cases in women. Pregnancy is not a common cause of SCAD When ACS occurs in the peripartum period, SCAD is responsible in 43% of cases. A study by Hassan et al. A study by Hassan et al. Lobo et al. The SCAD cases in Lobo et al.
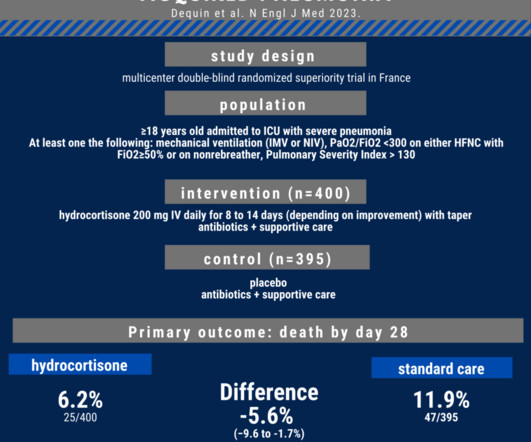
References: Metlay JP, Waterer GW, Long AC, et al. ESCAPe found no benefit in their trial of a continuous infusion of methylprednisolone in severely ill patients with CAP). In this podcast episode, we review a new multicenter randomized trial of hydrocortisone in severe CAP.
References: Ross RK, Kinlaw AC, Herzog MM, Funk MJ, Gerber JS. PMID: 27940800 Hersch AL, Gerber JS, Hicks LA, Pavia AT. However, Fluroquinolone resistance is increasing, so they should only be used if absolutely necessary! Nobody wants a pseudomonas superbug becoming prevalent! Pediatrics. 147(6):e202003316. Pediatr Infect Dis J.
Here is an article I wrote: Updates on the ECG in ACS. In left main occlusion, by blocking flow to both the anterior wall (LAD) and posterior wall (circ), the ST depression of posterior ischemia could theoretically diminish the ST elevation of anterior ischemia and leave only V1 with significant ST elevation (Nikus, et al. see below).
See this study showing an association between morphine and mortality in ACS: Use of Morphine in ACS is independently associated with mortality, at odds ratio of 1.4. de Winter et al in N Engl J Med 359:2071-2073, 2008. See this case: A man his 50s with chest pain.
References Go AS, Mozaffarian D, Roger VL, et al. Larribau R, Deham H, Niquille M, et al. Margey R, Browne L, Murphy E, et al. Kudenchuk PJ, Brown SP, Daya M, et al. Spies DM, Kiekenap J, Rupp D, et al. Holmén J, Hollenberg J, Claesson A, et al. Yannopoulos D, Bartos J, Raveendran G, et al.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content