This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
PMID: 32644703 Robinson PM, Griffiths E, Watts AC. PMID: 27227986 Glover NM, Black AC, Murphy PB. Commentary on an article by Marc Schnetzke, MD, et al.: “Determination of Elbow Laxity in a Sequential Soft-Tissue Injury Model. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. Simple elbow dislocation. 2023 Nov 5.
Studies such as those by Moise et al 14 and Ellis et al 39 have shown that the relative risk of developing an acute myocardial infarction in the territory supplied by an artery with a 70%. For more on MINOCA — See My Comment in the November 16, 2023 post in Dr. Smith's ECG Blog ).
IMPRESSION: The finding of sinus bradycardia with 1st-degree AV block + marked sinus arrhythmia + the change in PR interval from beat #5-to-beat #6 — suggests a form of vagotonic block ( See My Comment in the October 9, 2020 post in Dr. Smith's ECG Blog ). As a result — an ICD may need to be considered in selected cases.
What Your Gut Says: The patient has a tachydysrhythmia which may be the presentation of acute coronary syndrome (ACS) even though the patient has no ischemic symptoms. If the patient continues to have symptoms concerning for ACS, troponin testing should be pursued. SVT is not a presenting dysrhythmia consistent w/ ACS.
In fact, Kosuge et al. Stein et al. This is a paper worth reading : Marchik et al. Kosuge et al. showed that , when T-waves are inverted in precordial leads, if they are also inverted in lead III and V1, then pulmonary embolism is far more likely than ACS. Witting et al. of patients with PE and 3.3%
REBEL Cast Ep114 – High Flow O2, Suspected ACS, and Mortality? Click here for Direct Download of the Podcast Paper: Stewart, RAH et al. PMID: 33653685 Clinical Question: Is there an association between high flow supplementary oxygen and 30-day mortality in patients presenting with a suspected acute coronary syndrome (ACS)?
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). ACS and hyperkalemia both have lethal downstream consequences, so it is imperative for the clinician to acclimate to the presentation, or developing, features of each. link] [1] Zachary et al. 2] Costanzo, L.
VS abnormalities can drive this as well Strongly consider reversal of AC (this will typically come after control) Stopping the Bleeding PPE: these things bleed like stink. EMRAP HD: Epistaxis Posterior Pack References Cassisi NJ et al. PMID: 5569677 Zeyyan E et al. PMID: 20938948 Loftus BC et al.
Click here for Direct Download of the Podcast Paper: Aykan AC et al. References: Jaff MR et al. PMID: 21422387 Wan S et al. PMID: 15262836 Sharifi M et al. PMID: 27422214 Wang C et al. PMID: 19741062 Kucher N et al. PMID: 24226805 Piazza G et al. PMID: 26315743 Tapson VF et al.
Full blog post here. 100% seems too good to be true Morello et al., PMID: 39461792 Bottom line: The WOMAN 2 trial is a large double-blind RCT that shows no benefit of TXA in the prevention of postpartum hemorrhage, which fits with all of the existing literature demonstrating no role for TXA in the management of postpartum hemorrhage.
Dedicated followers of the Smith ECG Blog know that the STD of true subendocardial ischemia does not localize, yet some of the examples listed below demonstrate the opposite, and were subsequently labeled “diffuse ischemia” or “generic subendocardial changes” as a diagnosis of convenience. However, the maximal STD in this case is V3.
Article: Vaeli Zadeh A, Wong A, Crawford AC, Collado E, Larned JM. Kuttab et al’s findings, constituting 45% of the review’s weight, suggest that administering <30cc/kg IVF is associated with increased odds of mortality, delayed hypotension, and increased ICU utilization. times more intubations and 2.15
Brief aside: "Early repolarization" is a frequently proclaimed and poorly understood electrocardiographic phenomenon which mostly serves to reassure clinicians that not all ST elevations are ischemic (something readers of this blog know well). It relies on an 1 mm cut point, which this blog does not favor as an approach to ECG.
Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. Lindahl et al. From Gue at al. Most studies examine undifferentiated ACS cohorts, with only a handful providing separate data.
You can find more details in the full blog post. PECARN looks at probiotics for toddlers diarrhea… Schnadower D, Tarr PI, Casper TC, Gorelick MH, Dean JM, O’Connell KJ, Mahajan P, Levine AC, Bhatt SR, Roskind CG, Powell EC, Rogers AJ, Vance C, Sapien RE, Olsen CS, Metheney M, Dickey VP, Hall-Moore C, Freedman SB.
Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1] Amsterdam et al. Alencar et al. Lupu et al. Herman, Meyers, Smith et al. But only 6.4% link] References 1.
Thus, these troponins are very concerning for ACS, and subsequent ones will probably be diagnostic of acute MI. Evidence regarding intervention to non-culprit plaques is mixed and beyond the scope of this blog post. Heitner et al. Thus, one considers a test result that varies by 2 or less to be the same result.
This has been discussed many times before on this blog. In-depth discussion is beyond the scope of this blog. Similarly, the OMI paradigm respects ACS as a dynamic process in which ECG changes reflect the phase of myocardial injury and risk stratify which patients may benefit from emergent PCI. Bigger et al.
Methodology: 3/5 Usefulness: 1/5 Georgiopoulos G, et al. 2023 Oct 1;8(10):946-956 Question: Does the modified GRACE score incorporating continuous troponin improve ACS risk prediction? The post Modification of the GRACE Risk Score for Risk Prediction in Patients With Acute Coronary Syndromes appeared first on EMOttawa Blog.
Because there was proven thrombus (ACS) but the troponin never went above the 99% reference range (and therefore cannot be called MI -- definition of MI requires rise and/or fall of troponin with at least one value above the 99% reference range), this is UNSTABLE ANGINA with ST Elevation. A picture is worth 1,000 words.
But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. Dialysis patients have a high rate of ACS without chest pain and high rate of delayed diagnosis and delayed reperfusion 2.
Follow up with the dentist in the morning Reinsert the tooth and avoid solid food Reinsert the tooth and stabilize it with a bridge Remove the tooth and repair the gingival laceration Remove the tooth and wrap it in saline-soaked gauze FOR THE RIGHT ANSWER CLICK ON THE ROSH REVIEW LOGO BELOW References Day PF, Flores MT, O’Connell AC, et al.
Read More First10EM: Imaging for Renal Colic SGEM : SGEM XTRA: COME TOGETHER, RIGHT NOW – OVER RENAL COLIC References Chang, Helena, et al. Moore CL, Carpenter CR, Heilbrun ME, et al. Smith-Bindman R, Aubin C, Bailitz J, et al. PMID: 25229916 DOI: 10.1056/NEJMoa1404446 Westphalen AC, Hsia RY, Maselli JH, Wang R, Gonzales R.
In our opinion it should not be given in ACS unless you are committed to the cath lab. Learning Point: Any NSTEMI patient with active ongoing ACS symptoms refractory to medical management is supposed to go to the cath lab within 2 hours if available, per all guidelines in world, regardless of ECG findings. Am J Emerg Med.
There were zero patients in this study with a "normal" ECG who had any kind of ACS! Deutch et al. This defies all previous data on acute MI which would show that even undetectable troponins do not have a 100% negative predictive value. So this study is actually worthless. West J Emerg Med 2024).
Anecdotally, had there been symptoms unequivocally consistent with ACS then one could justifiably make the case for a potential D1 occlusion. Figure 2-1 The V1 / V2 leads were appropriately placed in this circumstance, and dedicated followers of the Smith ECG Blog will instantly recognize the problem at hand. 4] Baranchuk, A, et al.
Some providers were worried about ACS because of this ECG. My answer alleviated their concern for ACS and no further workup was done for ACS. Kosuge et al. showed that , when T-waves are inverted in precordial leads, if they are also inverted in lead III and V1, then pulmonary embolism is far more likely than ACS.
Smith: If this is ACS (a big if), t his is just the time when one should NOT use "upstream" dual anti-platelet therapy ("upstream" means in the ED before angiography). History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. Knotts et al.
Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS. I have posted previous such cases, but in searching my own blog, I could not find them. The ECG only tells you there is ischemia, not the etiology of it.
The cath report showed: Significant stenosis with subtotal occlusion (99%) in the prox to mid Lcx, culprit of ACS, TIMI flow 1. Available from: [link] If you are wondering about the Barcelona rule, then you should read the above paper by Khawaja et al. Cardiac catheterization occurred around 1pm (18 hours after arrival). 2021;23:187.
link] Shvilkin et al. Thus, the very well informed physician could differentiate these ECGs from those of an LBBB patient with MI: 1) no concordance 2) no excessive discordance 3) LBBB with tachycardia, probably rate related 4) subsequent T wave inversion that, according to Shvilkin et al., is diagnostic of cardiac memory.
MOREVER, the morphology of the TWI is just not right for ACS. S1Q3T3 This is a paper worth reading : Marchik et al. Kosuge et al. showed that, when T-waves are inverted in precordial leads, if they are also inverted in lead III and V1, then pulmonary embolism is far more likely than ACS. inverted T-waves in V1 and V2, 1.8;
SCAD isn’t rare, especially in women Historically SCAD had been identified in 22% of ACS cases in women. Pregnancy is not a common cause of SCAD When ACS occurs in the peripartum period, SCAD is responsible in 43% of cases. A study by Hassan et al. A study by Hassan et al. Lobo et al. The SCAD cases in Lobo et al.
Previously, I wrote a blog on pre-oxygenation, referencing my personal “weapon of choice” as chosen from the 7 Ps of RSI. But, putting them both into one blog would make for a read far too long to maintain even my attention span (which honestly is pretty short). And according to a paper from Russotto et al.
It is also true that anterior and inferior T-wave inversion could be consistent with reperfusion of a type III wraparound LAD occlusion, despite the fact that Kosuge et al showed that T-wave inversion in lead III is much more likely to be PE than ACS if your differential contains nothing else. Stein et al. Kosuge et al.
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al. Lindahl et al. From Gue at al.
But if they do present: The very common presentation of diffuse STD with reciprocal STE in aVR is NOT left main occlusion , though it might be due to sub total LM ACS, but is much more often due to non-ACS conditions, especially demand ischemia. Widimsky P et al. Knotts et al. TIMI 0/1 flow).(61,62)
See this study showing an association between morphine and mortality in ACS: Use of Morphine in ACS is independently associated with mortality, at odds ratio of 1.4. de Winter et al in N Engl J Med 359:2071-2073, 2008. See this case: A man his 50s with chest pain.
Here is an article I wrote: Updates on the ECG in ACS. In left main occlusion, by blocking flow to both the anterior wall (LAD) and posterior wall (circ), the ST depression of posterior ischemia could theoretically diminish the ST elevation of anterior ischemia and leave only V1 with significant ST elevation (Nikus, et al. see below).
Lemkes et al. No wall motion abnormality This shows that significant ACS can have ZERO WMA!! If you are prepared for this, they conclude that it is acceptable to wait until the morning for intervention. The Proximal LAD thrombus lysed or partially lysed, restoring flow. Eur Heart J 2018. Full text link.
In this case, the patient had failed to take his atenolol in the AM and was having reflex tachycardia in addition to ACS. If there is ST depression (as there is here), it is ACS. Conversely, Matetzky et al. Kligfield P, Gettes LS, Bailey JJ, et al. Matetzky S, Friemark D, Feinberg MS, et al. BP was 160/100.
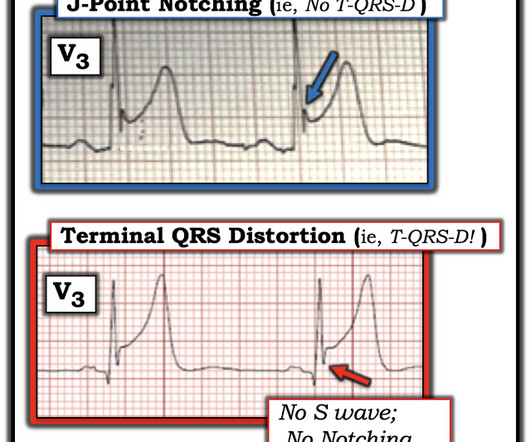
It was shown to me with worry for ischemic ST elevation, which is certainly possible from severe CO toxicity, or concomitant ACS. Yelken B et al. There are an increasing number of other examples of what T-QRS-D is, and what it is not on Dr. Smiths Blog. MORE PRACTICE = 4 examples ( 3 positive; 1 not for T-QRS-D ).
In the December 5, 2022 post of Dr. Smith's ECG Blog — We show 4 additional cases of this pulse-tap artifact. Additional review of ECG artifacts by Pérez-Riera et al ( Ann Noninvasic Electrocardiol 23:e12494, 2018 ) VT Artifact — by Knight et al: NEJM 341:1270-1274, 1999. This is no longer the case!
Paper: Mason JM, et al. These results were corroborated with other another study by Gritensko et al. Sepsis, hyperthyroidism, dehydration, heart failure, ACS, etc). References Mason JM, et al. 2018, PMID: 30571262 Gritsenko, Diana, et al. Link to Paper Here Shojaee M, et al. Am J Emerg Med. Am J Emerg Med.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content