

Formula Utilization
EMS 12-Lead
JUNE 20, 2022
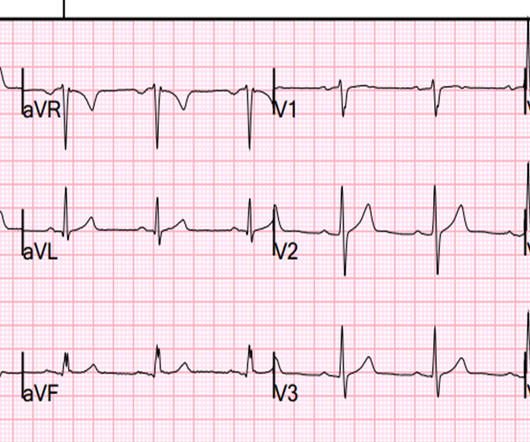
Moreover, he had no pertinent medical history to report in terms of CAD, HTN, HLD, or DM, for example. Although the attending crews did not consider the ECG pathognomonic for occlusive thrombosis, they nonetheless considered the patient high-risk for ACS and implored him to reconsider. A 12 Lead ECG was recorded. 2] Driver, B.



















Let's personalize your content