This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Studies such as those by Moise et al 14 and Ellis et al 39 have shown that the relative risk of developing an acute myocardial infarction in the territory supplied by an artery with a 70%. years, with the interval as long as 12 or 18 years in some studies. Unfortunately, vascular remodeling is variable and inconsistent.
Intermediate-risk patients may be further stratified based on recent stress testing or coronary angiogram findings plus a modified HEART or Emergency Department Assessment of Chest Pain (EDACS) score. The patient has no previous stress testing or coronary angiogram, and he is not low risk by HEART or EDACS scoring.
Date: September 23, 2024 Reference: Essat et al. The patient has no specific risk factors for acute coronary syndrome (ACS) or dissection. Reference: Essat et al. Diagnostic Accuracy of D-Dimer for Acute Aortic Syndromes: Systematic Review and Meta-Analysis.
Date: June 30th, 2022 Reference: McGinnis et al. Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Date: June 30th, 2022 Reference: McGinnis et al. Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Reference: McGinnis et al.
Why Was Cardiac Cath Negative for Coronary Disease? As noted by Dr. Nossen — this patient qualified as MINOCA ( M yocardial I nfarction with N on- O bstructive C oronary A rteries ) — since troponin was positive on his 2nd admission, yet there was no evidence of obstructive coronary disease on cath.
What Your Gut Says: The patient has a tachydysrhythmia which may be the presentation of acute coronary syndrome (ACS) even though the patient has no ischemic symptoms. Essentially, we are using the troponin assay to find patients with ACO who may be benefited by coronary interventions or risk factor modification.
Date: January 16th, 2020 Reference: Troponin Testing and Coronary Syndrome in Geriatric Patients With Nonspecific Complaints: Are We Overtesting? Date: January 16th, 2020 Reference: Troponin Testing and Coronary Syndrome in Geriatric Patients With Nonspecific Complaints: Are We Overtesting? Reference: Wang et al.
Date: September 8th, 2021 Reference: Desch et al. Date: September 8th, 2021 Reference: Desch et al. Defibrillation is the treatment of choice in these cases but does not often result in sustained ROSC ( Kudenchuk et al 2006). Acute coronary syndrome (ACS) is responsible for the majority (60%) of all OHCAs in patients.
Although the attending crews did not consider the ECG pathognomonic for occlusive thrombosis, they nonetheless considered the patient high-risk for ACS and implored him to reconsider. One cannot rely on this feature as a means of detecting changes – subtle, or dramatic – for volatile occlusive coronary thrombus. 2] Driver, B.
In fact, Kosuge et al. showed that among patients with either acute coronary syndrome or acute pulmonary embolism and negative T waves in the precordial leads (V1-V4), that inverted T waves in leads III and V1 were present in only 1% of patients with acute coronary syndrome and 88% of patients with pulmonary embolism. “The
Background: Historically, we have treated acute coronary syndrome with supplemental oxygen regardless of the patient ’ s oxygen saturation. More recent evidence, however, demonstrates that too much oxygen could be harmful ( AVOID Trial ) by causing coronary vasoconstriction and increasing oxidative stress. Low O2 protocol: 3.1%
Myth 1 Absence of Classic Chest Pain obviates the need for ACS work up The absence of chest pain in no way excludes the diagnosis of ACS. Around 33-50% of the patients with ACS present to the hospital without chest pain. References: Canto JG, Shlipak MG, Rogers WJ, et al. Dorsch MF, Lawrence RA, Sapsford RJ, et al.
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). ACS and hyperkalemia both have lethal downstream consequences, so it is imperative for the clinician to acclimate to the presentation, or developing, features of each. link] [1] Zachary et al.
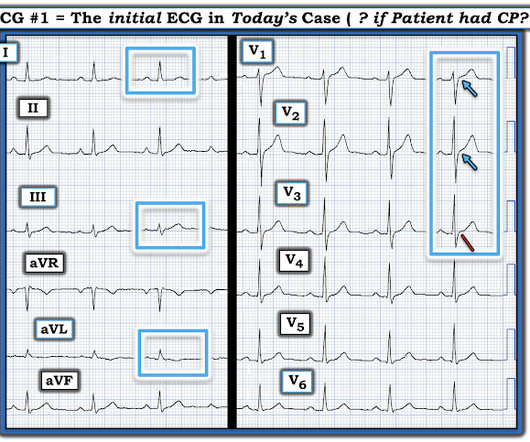
There is appreciable STE aVR with near-global STD that appropriately maximizes in Leads II and V5, and thus suggesting a circumstance of generic, diffusely populated, circumferential subendocardial ischemia versus occlusive coronary thrombus. [1] It’s judicious, then, to arrange for coronary angiogram. link] [1] Mirand, D.
The ECG is just a test: a Bayesian approach to acute coronary occlusion If a patient with a recent femur fracture has sudden onset of pleuritic chest pain, shortness of breath, and hemoptysis, the D-dimer doesn’t matter: the patient’s pre-test likelihood for PE is so high that they need a CT. Amsterdam et al. Alencar et al.
Methodology: 3/5 Usefulness: 1/5 Georgiopoulos G, et al. 2023 Oct 1;8(10):946-956 Question: Does the modified GRACE score incorporating continuous troponin improve ACS risk prediction? The post Modification of the GRACE Risk Score for Risk Prediction in Patients With Acute Coronary Syndromes appeared first on EMOttawa Blog.
Such findings would normally suggest primary ischemia with concomitant surveillance of coronary occlusion, but these ST/T changes might very well be secondary to the Escape mechanism at hand. Evaluation of T-wave morphology in patients with left bundle branch block and suspected acute coronary syndrome. 3] Meyers, H. 4] Dodd, K.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" She had a proven 100% Left Main occlusion No ST shift in aVR This pattern of RBBB/LAFB was also the most common pattern in Fiol et al.
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction. This is not the case.
Cardiology admitted him for observation with plans for next-day coronary angiogram. Smith and Meyers found that patients presenting with high-risk ACS and any ST-depression, even less than 1 mm, maximal in leads V1-V4 to be 97% specific for OMI and 96% specific for OMI requiring emergent PCI. [5] 1] Driver, B. 2] van Gorselen, E.,
Note that as many as 7% of patients with acute coronary syndrome have chest pain reproducible on palpation [Lee, Solomon]. which reduces the pre-test probability of acute coronary syndrome by less than 30% [McGee]. The original term " benign early repolarization" has fallen out of favor since the seminal paper by Haïssaguerre et al.
Click here for Direct Download of the Podcast Paper: Aykan AC et al. References: Jaff MR et al. PMID: 21422387 Wan S et al. PMID: 15262836 Sharifi M et al. PMID: 27422214 Wang C et al. PMID: 19741062 Kucher N et al. PMID: 24226805 Piazza G et al. PMID: 26315743 Tapson VF et al.
Date: May 24th, 2022 Reference: Broder et al. Date: May 24th, 2022 Reference: Broder et al. Reference: Broder et al. Guidelines for Reasonable and Appropriate Care in the Emergency Department (GRACE) 2: Low-Risk, Recurrent Abdominal Pain in the Emergency Department.
Notoriously elusive, with a high misdiagnosis rate, thoracic aortic dissection (AD) can mimic many conditions, including acute coronary syndrome (ACS, the most common), gastroesophageal reflux disease (GERD), stroke, and spinal-cord compression. ACS is the most common misdiagnosis and often leads to inappropriate anticoagulation.
There were zero patients in this study with a "normal" ECG who had any kind of ACS! Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. Deutch et al. So this study is actually worthless.
Serial ECGs enhance the diagnosis of acute coronary syndrome. Similarly, the OMI paradigm respects ACS as a dynamic process in which ECG changes reflect the phase of myocardial injury and risk stratify which patients may benefit from emergent PCI. Bigger et al. Sadowski ZP, Alexander JH, Skrabucha B, et al.
In our opinion it should not be given in ACS unless you are committed to the cath lab. Learning Point: Any NSTEMI patient with active ongoing ACS symptoms refractory to medical management is supposed to go to the cath lab within 2 hours if available, per all guidelines in world, regardless of ECG findings. 2009;95:1701–1706.
Smith: If this is ACS (a big if), t his is just the time when one should NOT use "upstream" dual anti-platelet therapy ("upstream" means in the ED before angiography). History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. Anything more on history?
Many conditions outside of acute coronary syndrome (ACS) mimic ST-elevation myocardial infarction (STEMI), but only a handful of cases have reported ST-elevations (STE) in the setting of pancreatic inflammation where underlying ACS was excluded. 2 Proposed hypothesis as described by Hsu et al.,
He reported a history of ischemic cardiomyopathy with coronary stent placement approximately 10 years prior, but could not recall the specific artery involved. Anecdotally, had there been symptoms unequivocally consistent with ACS then one could justifiably make the case for a potential D1 occlusion. 4] Baranchuk, A, et al.
The biphasic T wave is consistent with recent reperfusion of an occluded coronary artery supplying the inferior region. Here’s the angiogram of the RCA : No thrombus or plaque rupture in the RCA (or any coronary artery) was found. This MI wasn’t caused by a ruptured plaque of CAD - it was a coronary artery dissection of the RCA.
Thus, these troponins are very concerning for ACS, and subsequent ones will probably be diagnostic of acute MI. Heitner et al. We know that even high-sensitivity troponin may not exceed the "normal" range for a period of hours in certain patients with acute coronary occlusion. DOI:10.1161/CIRCINTERVENTIONS.118.007305),
-See this study showing an association between morphine and mortality in ACS: Use of Morphine in ACS is independently associated with mortality, at odds ratio of 1.4. Association of intravenous morphine use and outcomes in acute coronary syndromes: Results from the CRUSADE Quality Improvement Initiative.
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al. One need not have obstructive coronary disease to have occlusive thrombus!
Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS. The case I presented in My Comment to that March 9, 2020 post showed a patient with this pattern — who on cath had no more than minimal coronary disease.
But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. Dialysis patients have a high rate of ACS without chest pain and high rate of delayed diagnosis and delayed reperfusion 2.
Armstrong et al. The patient has also developed sinus bradycardia, which may result from right coronary artery ischemia to the SA node. Angiogram showed a culprit lesion of 100% stenosis to the right coronary artery and 100% stenosis of the right posterior descending artery, both with TIMI 0 flow. Just another NSTEMI.
Here is an article I wrote: Updates on the ECG in ACS. In left main occlusion, by blocking flow to both the anterior wall (LAD) and posterior wall (circ), the ST depression of posterior ischemia could theoretically diminish the ST elevation of anterior ischemia and leave only V1 with significant ST elevation (Nikus, et al. see below).
A 68-year-old male with a past medical history of hypertension, diabetes mellitus, and coronary artery disease with a drug eluting stent placed 2 months ago presents with dizziness and vomiting that began 3 hours ago. The NIHSS cutoff that predicts outcomes is 4 points higher in AC compared with PC infarctions. Arch Neurol.
It is our job to identify this entity and ensure these patients receive the same care they would for a STEMI in any other coronary artery territory. Therein lies the limitation of electrocardiography in diagnosing acute coronary occlusion. Matetzky S, Friemark D, Feinberg MS, et al. O'Gara et al. O'Gara et al.
The diagnostic coronary angiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aortic valve. Author continued : STE in aVR is often due to left main coronary artery obstruction (OR 4.72), and is associated with in-hospital cardiovascular mortality (OR 5.58).
Lemkes et al. No wall motion abnormality This shows that significant ACS can have ZERO WMA!! A comparison of electrocardiographic changes during reperfusion of acute myocardial infarction by thrombolysis or percutaneous transluminal coronary angioplasty. The Proximal LAD thrombus lysed or partially lysed, restoring flow.
In this case, the patient had failed to take his atenolol in the AM and was having reflex tachycardia in addition to ACS. If there is ST depression (as there is here), it is ACS. Smith SW as editor of section on Acute Coronary Syndromes). Conversely, Matetzky et al. Kligfield P, Gettes LS, Bailey JJ, et al.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















































Let's personalize your content