This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Bupe Allergy Buprenorphine induction has been the mainstay of emergencydepartment treatment of opioid use disorder for more than a decade [11, 12]. Multimodal medication options for fentanyl-xylazine withdrawal management in London et al. DOI: Papudesi BN, Malayala SV, Regina AC. D’Onofrio G, Hawk KF, Perrone J, et al.
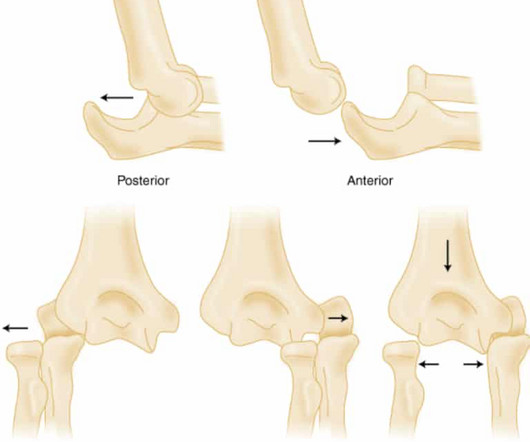
Trauma season is at hand and like all other pediatric emergencydepartments in the country, we find our ED breaking ( pun intended ) at the seams with orthopedic injuries. Davidson JS, Brown DJ, Barnes SN, et al. Pediatr Emerg Care. West S, Andrews J, Bebbington A, et al. Symons S, Rowsell M, Bhowal B, et al.
You turn to the attending and ask, “do you really think this could be acute coronary syndrome (ACS)?” Background: Patients 65 years and older account for about 15% of emergencydepartment visits in the United States. Reference: Wang et al. The proportion of patients with ACS at the index visit or within 30 days. *
Chris Bond is an emergency medicine physician and assistant Professor at the University of Calgary. Reference: Brichko et al. Reference: Brichko et al. Rapid Administration of Methoxyflurane to Patients in the EmergencyDepartment (RAMPED): A Randomised controlled trial of Methoxyflurane vs Standard care.
Date: September 8th, 2021 Reference: Desch et al. Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. first appeared on The Skeptics Guide to Emergency Medicine. Date: September 8th, 2021 Reference: Desch et al.
Date: June 30th, 2022 Reference: McGinnis et al. Guest Skeptic: Dr. Corey Heitz is an emergency physician in Roanoke, Virginia. He is also the CME editor for Academic Emergency Medicine. Date: June 30th, 2022 Reference: McGinnis et al. Guest Skeptic: Dr. Corey Heitz is an emergency physician in Roanoke, Virginia.
Date: May 24th, 2022 Reference: Broder et al. Guidelines for Reasonable and Appropriate Care in the EmergencyDepartment (GRACE) 2: Low-Risk, Recurrent Abdominal Pain in the EmergencyDepartment. Date: May 24th, 2022 Reference: Broder et al. Reference: Broder et al.
It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). ACS and hyperkalemia both have lethal downstream consequences, so it is imperative for the clinician to acclimate to the presentation, or developing, features of each. link] [1] Zachary et al. 2] Costanzo, L.
Background Information: Atrial fibrillation with rapid ventricular rate (RVR) is one of the many tachydysrhythmias we encounter in the EmergencyDepartment (ED). Paper: Mason JM, et al. Amiodarone versus digoxin for acute rate control of atrial fibrillation in the emergencydepartment. Am J Emerg Med.
It is commonly used in EmergencyDepartments, especially in febrile and possibly infectious patients. ACS and Aortic Dissection - For ACS and Dissection, the higher CRP levels, the worse prognosis. It is not used to diagnose ACS/Dissection. Utility of CRP 1. Intensive Care Med2002; 28(6): 740-745.
The parents of 18-month-old Susie brought her to the EmergencyDepartment after she had a seizure at home. doi:10.1093/tropej/fmz071 Expert Panel on Pediatric Imaging, Trofimova A, Milla SS, et al. 2019-0134 Hirtz D, Ashwal S, Berg A, et al. Seizure patient selection for emergency computed tomography. Pediatr Rev.
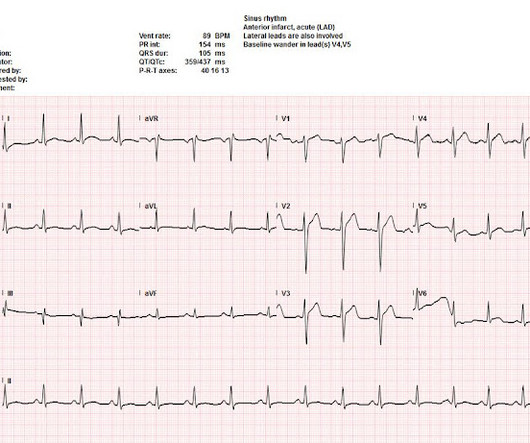
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. Upon arrival to the emergencydepartment, a senior emergency physician looked at the ECG and said "Nothing too exciting." Lindahl et al.
There are greater than 2 million annual emergencydepartment visits for suspected renal colic in the US, and Ct scanning is performed for more than 90% of patients who receive a diagnosis of kidney stone. Moore CL, Carpenter CR, Heilbrun ME, et al. Am J Emerg Med. Smith-Bindman R, Aubin C, Bailitz J, et al.
Antonaci L, et al. Tritos NA, et al. Levi M, et al. Fishbein MH, et al. Cetinkaya PG, et al. Niu T, et al. Verkuijl SJ, et al. Varni JW, et al. Dias FC, et al. Peter C, et al. Ahlberg R, et al. Shir A, et al. Kuypers KLAM, et al. Hegeman EM, et al.
, tells us that we physicians do not need to even look at this ECG until the patient is placed in a room because the computer says it is normal: Validity of Computer-interpreted “Normal” and “Otherwise Normal” ECG in EmergencyDepartment Triage Patients I reviewed this article for a different journal and recommended rejection and it was rejected.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergencydepartment with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. Amsterdam et al. Alencar et al. Lupu et al. Herman, Meyers, Smith et al. But only 6.4%
Written by Willy Frick A man in his 50s with a history of hypertension, dyslipidemia, type 2 diabetes mellitus, and prior inferior OMI status post DES to his proximal RCA 3 years prior presented to the emergencydepartment at around 3 AM complaining of chest pain onset around 9 PM the evening prior.
The NIHSS cutoff that predicts outcomes is 4 points higher in AC compared with PC infarctions. References: Gaillard F, Glick Y, Tatco V, et al. 61.4.496 Navi BB, Kamel H, Shah MP, et al. Application of the ABCD2 score to identify cerebrovascular causes of dizziness in the emergencydepartment. Arch Neurol.
Many conditions outside of acute coronary syndrome (ACS) mimic ST-elevation myocardial infarction (STEMI), but only a handful of cases have reported ST-elevations (STE) in the setting of pancreatic inflammation where underlying ACS was excluded. 2 Proposed hypothesis as described by Hsu et al., Yu ES, Lange JJ, Broor A, et al.
Smith: If this is ACS (a big if), t his is just the time when one should NOT use "upstream" dual anti-platelet therapy ("upstream" means in the ED before angiography). History sounds concerning for ACS (could be critical stenosis, triple vessel), but differential also includes dissection, GI bleed, etc. Knotts et al.
A 35-year-old male presented to the emergencydepartment complaining of chest pain that started 1.5 5 Studies looking at this phenomenon in the emergencydepartment setting for patients presenting with chest pain are lacking. Dr. Young is an emergency physician at Saint Francis Hospital and Medical Center, Hartford, Conn.
A 67-year-old man presents to the emergencydepartment (ED) in cardiac arrest. References Go AS, Mozaffarian D, Roger VL, et al. Larribau R, Deham H, Niquille M, et al. Margey R, Browne L, Murphy E, et al. Kudenchuk PJ, Brown SP, Daya M, et al. Spies DM, Kiekenap J, Rupp D, et al. Circulation.
He had no symptoms of ACS. The remainder of his EmergencyDepartment stay was uneventful. Here is the clinical informaton on ECG 2: A man in his 50s presented to the EmergencyDepartment with acute chest pain that started within the past few hours. de Winter et al in N Engl J Med 359:2071-2073, 2008.
Here is a video lecture of subtle LAD occlusion: One hour lecture on Subtle ECG Findings of Coronary Occlusion The 3-variable formula comes from this paper: Smith SW et al. Annals of Emergency Medicine 2012;60:45-56. The 4-variable formula is based on this paper: Driver, BE et al. 4-variable version still to come.
Intermediate-risk patients may be further stratified based on recent stress testing or coronary angiogram findings plus a modified HEART or EmergencyDepartment Assessment of Chest Pain (EDACS) score. References Writing Committee, Kontos MC, de Lemos JA, et al. 2022.08.750 Collet JP, Thiele H, Barbato E, et al.
Date: September 23, 2024 Reference: Essat et al. Annals of Emergency Medicine, May 2024 Guest Skeptic: Dr. Casey Parker is a Rural Generalist from Australia who is also an ultrasounder. The patient has no specific risk factors for acute coronary syndrome (ACS) or dissection. Reference: Essat et al.
Diarrhea is one of the most common complaints in the pediatric emergencydepartment, especially in the summer and early fall. Predicting Adverse Outcomes for Shiga Toxin-Producing Escherichia coli Infections in EmergencyDepartments. Schnadower, D., Finkelstein, Y.,Desai, Bergmann, K., Hariharan, S., 2021 May;232:200-206.e4.
Date: May 23rd, 2019 Reference: Joseph et al. Guest Skeptic: Dr. Robert Edmonds is an emergency physician in the US Air Force in Virginia. DISCLAIMER: THE VIEWS AND OPINIONS OF THIS PODCAST DO NOT […] The post SGEM#258: REBOA, Re-Re-Re-REBOA first appeared on The Skeptics Guide to Emergency Medicine. Reference: Joseph et al.
Written by Bobby Nicholson, MD 67 year old male with history of hypertension and hyperlipidemia presented to the EmergencyDepartment via ambulance with midsternal nonradiating chest pain and dyspnea on exertion. In fact, Kosuge et al. Stein et al. This is a paper worth reading : Marchik et al. Kosuge et al.
Robert Edmonds is an emergency medicine physician in the Air Force in Dayton, Ohio, and a University of Missouri-Kansas City residency alumni from 2016. Reference: Jhunjhunwala et al. Journal of Trauma and […] The post SGEM#332: Think Outside the Cardiac Box first appeared on The Skeptics Guide to Emergency Medicine.
Myth 1 Absence of Classic Chest Pain obviates the need for ACS work up The absence of chest pain in no way excludes the diagnosis of ACS. Around 33-50% of the patients with ACS present to the hospital without chest pain. References: Canto JG, Shlipak MG, Rogers WJ, et al. Dorsch MF, Lawrence RA, Sapsford RJ, et al.
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergencydepartment with 2 days of heavy substernal chest pain and nausea. Bigger et al. Annals of Emergency Medicine , 31 (1), 3–11. Sadowski ZP, Alexander JH, Skrabucha B, et al. Leave it alone.
Compare this with the Panickar et al. Fortunately, Lee et al. Lee B, Turner S, Borland M, Csonka P, Grigg J, Guilbert TW, et al. Future of Pre-School Wheeze Whilst Lee et al. Cronin JJ, McCoy S, Kennedy U, An Fhailí SN, Wakai A, Hayden J, et al. Annals of Emergency Medicine. study from 200 9.
References: Heffner AC et al. Incidence and factors associated with cardiac arrest complicating emergency airway management. PMID: 23911630 Kim WY et al. actors Associated with the Occurrence of Cardiac Arrest after Emergency Tracheal Intubation in the EmergencyDepartment. Int J Emerg Med.
Such aggressive investigation was particularly warranted in this case because of symptoms compatible with ACS, as well as an equally frightening revelation of family history. New insights into the use of the 12 Lead Electrocardiogram for diagnosing Acute Myocardial Infarction in the emergencydepartment. link] [1] Mirand, D.
Fournier gangrene: an histori9]al reappraisal. MD Diagnosis: Fournier's Gangrene, Emergency Medicine News: May 2005 - Volume 27 - Issue 5 - p 36. Sugihara T, Yasunaga H, Horiguchi H, et al. Bjurlin MA, O'Grady T, Kim DY, et al. Sorensen MD, Krieger JN, Rivara FP, et al. Thwaini A, Khan A, Malik A, et al.
Notoriously elusive, with a high misdiagnosis rate, thoracic aortic dissection (AD) can mimic many conditions, including acute coronary syndrome (ACS, the most common), gastroesophageal reflux disease (GERD), stroke, and spinal-cord compression. The patient is admitted for ACS to a cardiologist who says he will see the patient in the morning.
Optimally, bystander CPR, including the administration of rescue breaths, should be initiated prior to arrival of emergency medical services. 3 Once the patient arrives in your emergencydepartment, a rapid review of the patient’s status and results of resuscitative efforts should be performed. Pediatr Emerg Med Pract.
Lactate Troponin Could this be ACS or myocarditis? Unanticipated death after discharge home from the emergencydepartment. Ann Emerg Med. 2006.11.018 Gabayan GZ, Sun BC, Asch SM, et al. Qualitative factors in patients who die shortly after emergencydepartment discharge. Acad Emerg Med.
Forestell B, Battaglia F, Sharif S, et al. Prekker ME, Bjorklund AR, Myers C, et al. Ann Emerg Med. This single-centre academic urban institution in the United States (US) undertook a 10-year retrospective observational study of paediatric intubation and bougie use in their emergencydepartment (ED). Resuscitation.
As recurrent ischaemia is the principle event reduced by early intervention in NSTE-ACS, these are important endpoint events occurring with delayed angiography and there is a consistent signal for harm now from two data sources.”[5] Kontos et al. Welsh et al. Busk et al. Eur Heart J 2009 4 Lemkes et al.
But if they do present: The very common presentation of diffuse STD with reciprocal STE in aVR is NOT left main occlusion , though it might be due to sub total LM ACS, but is much more often due to non-ACS conditions, especially demand ischemia. Widimsky P et al. Knotts et al. TIMI 0/1 flow).(61,62)
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content