This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Davidson JS, Brown DJ, Barnes SN, et al. West S, Andrews J, Bebbington A, et al. Symons S, Rowsell M, Bhowal B, et al. The post Rebaked Morsel: Pediatric Buckle and Greenstick Forearm Fractures appeared first on Pediatric EM Morsels. J Pediatr Orthop. 2018;Volume 00(00):DOI:10.1097/BPO.0000000000001169. 0000000000001169.
Case A patient arrives via EMS from the bus station complaining of fever, vomiting, and back pain. Our experience: It was not long ago that we instructed our staff that: ‘COWS >8, give ’em 8 (mg of buprenorphine).’ Multimodal medication options for fentanyl-xylazine withdrawal management in London et al. 2023 [book].
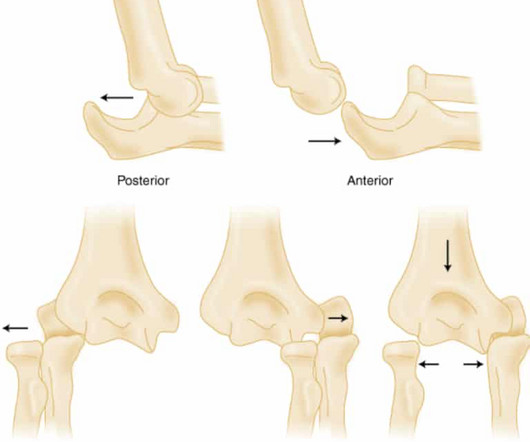
PMID: 32644703 Robinson PM, Griffiths E, Watts AC. PMID: 27227986 Glover NM, Black AC, Murphy PB. Commentary on an article by Marc Schnetzke, MD, et al.: “Determination of Elbow Laxity in a Sequential Soft-Tissue Injury Model. Treasure Island (FL): StatPearls Publishing; 2024 Jan–. Simple elbow dislocation. 2023 Nov 5.
Date: September 8th, 2021 Reference: Desch et al. Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. Date: September 8th, 2021 Reference: Desch et al. The TOMAHAWK Investigators. The TOMAHAWK Investigators.
We’ll keep it short, while you keep that EM brain sharp. The NIHSS cutoff that predicts outcomes is 4 points higher in AC compared with PC infarctions. References: Gaillard F, Glick Y, Tatco V, et al. 61.4.496 Navi BB, Kamel H, Shah MP, et al. link] Nael K, Khan R, Choudhary G, Meshksar A, Villablanca P, Tay J, et al.
According to the EMS narrative, this patient initially refused hospital transport and advised that he would seek evaluation at a later time with his personal physician. According to the EMS narrative, this patient initially refused hospital transport and advised that he would seek evaluation at a later time with his personal physician.
What Your Gut Says: The patient has a tachydysrhythmia which may be the presentation of acute coronary syndrome (ACS) even though the patient has no ischemic symptoms. If the patient continues to have symptoms concerning for ACS, troponin testing should be pursued. SVT is not a presenting dysrhythmia consistent w/ ACS.
REBEL Cast Ep114 – High Flow O2, Suspected ACS, and Mortality? Click here for Direct Download of the Podcast Paper: Stewart, RAH et al. PMID: 33653685 Clinical Question: Is there an association between high flow supplementary oxygen and 30-day mortality in patients presenting with a suspected acute coronary syndrome (ACS)?
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. In fact, Kosuge et al. Stein et al. This is a paper worth reading : Marchik et al. Kosuge et al. Witting et al. looked at consecutive patients with PE, ACS, or neither. What do you think?
The post Hemolytic Uremic Syndrome (HUS): Rebaked Morsel appeared first on Pediatric EM Morsels. Schnadower, D., Finkelstein, Y.,Desai, Bergmann, K., Hariharan, S., HUS and RRT in STEC-infected Children. 2021 May;232:200-206.e4. doi: 10.1016/j.jpeds.2020.12.077. 2020.12.077. Epub 2021 Jan 5. PMID: 33417918; PMCID: PMC8084908.
He presented to EMS with extreme pallor, Levine sign, diaphoresis, bilateral arm pain, and an apprehensive sense of doom. It should be emphasized here that this is a presentation of high-pretest probability for Acute Coronary Syndrome (ACS). In the case of ACS, the ECG can rapidly change from this. link] [1] Zachary et al.
VS abnormalities can drive this as well Strongly consider reversal of AC (this will typically come after control) Stopping the Bleeding PPE: these things bleed like stink. REBEL EM: Do Patients with Posterior Epistaxis Managed by Posterior Packs Require ICU Admission? EMRAP HD: Epistaxis Posterior Pack References Cassisi NJ et al.
He reported to EMS a medical history of GERD only. V2 – in the final EMS ECG the ST segment was baseline. V3 – in the final EMS ECG the ST segment was still slightly depressed. The EMS crews were correct moving forward with STEMI activation. However, in this context (i.e. 1] Driver, B. Emergency Medicine Journal, 1-5. [2]
Follow up with the dentist in the morning Reinsert the tooth and avoid solid food Reinsert the tooth and stabilize it with a bridge Remove the tooth and repair the gingival laceration Remove the tooth and wrap it in saline-soaked gauze FOR THE RIGHT ANSWER CLICK ON THE ROSH REVIEW LOGO BELOW References Day PF, Flores MT, O’Connell AC, et al.
Reference: Jhunjhunwala et al. Reference: Jhunjhunwala et al. The patient is an adult male with a gunshot wound to the chest, and they’re combative with emergency medical services (EMS). Reassessing the cardiac box: A comprehensive evaluation of the relationship between thoracic gunshot wounds and cardiac injury.
Click here for Direct Download of the Podcast Paper: Aykan AC et al. References: Jaff MR et al. PMID: 21422387 Wan S et al. PMID: 15262836 Sharifi M et al. PMID: 27422214 Wang C et al. PMID: 19741062 Kucher N et al. PMID: 24226805 Piazza G et al. PMID: 26315743 Tapson VF et al.
Date: May 24th, 2022 Reference: Broder et al. Date: May 24th, 2022 Reference: Broder et al. Reference: Broder et al. Guidelines for Reasonable and Appropriate Care in the Emergency Department (GRACE) 2: Low-Risk, Recurrent Abdominal Pain in the Emergency Department. There can be many presentations for low-risk abdominal pain.
Article: Vaeli Zadeh A, Wong A, Crawford AC, Collado E, Larned JM. Kuttab et al’s findings, constituting 45% of the review’s weight, suggest that administering <30cc/kg IVF is associated with increased odds of mortality, delayed hypotension, and increased ICU utilization. times more intubations and 2.15
Notoriously elusive, with a high misdiagnosis rate, thoracic aortic dissection (AD) can mimic many conditions, including acute coronary syndrome (ACS, the most common), gastroesophageal reflux disease (GERD), stroke, and spinal-cord compression. The patient is admitted for ACS to a cardiologist who says he will see the patient in the morning.
Reference: EM@3AM – Heat Stroke Case 2: 40-year-0ld female feels unwell but no other specific complaints. 2016 study published in American Journal of Emergency Medicine , “ Urinary obstruction is an important complicating factor in patients with septic shock due to urinary infection ” by Reyner et al. ROS unremarkable.
EMS finds him supine, alert and oriented, and without any gross distress. In isolation, however, syncope does not hold significant weight for OMI – as opposed to something like crushing chest discomfort, for example – although stereotypical ACS might become blurry in both the elderly and diabetic populations. 3] Meyers, H. 4] Dodd, K.
About 2 hours later the patient arrived at a PCI-capable center and repeat ECG was obtained: The transferring EMS crew noted “runs of VT” during transport. Similarly, the OMI paradigm respects ACS as a dynamic process in which ECG changes reflect the phase of myocardial injury and risk stratify which patients may benefit from emergent PCI.
PARAMEDIC 3 randomized 6,000 (but they were supposed to get to 15,000) patients with out of hospital arrest from multiple EMS agencies in the UK to either an IO or IV to start. PMID: 39480221 We have 2 studies looking at the same question published in the same edition of the NEJM, so I will tackle them together. ( of the IO group and 5.1%
Antonaci L, et al. Tritos NA, et al. Levi M, et al. Fishbein MH, et al. Cetinkaya PG, et al. Niu T, et al. Verkuijl SJ, et al. Varni JW, et al. Dias FC, et al. Peter C, et al. Ahlberg R, et al. Shir A, et al. Kuypers KLAM, et al. Hegeman EM, et al.
Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1] Amsterdam et al. Alencar et al. Lupu et al. Herman, Meyers, Smith et al. But only 6.4% link] References 1.
EMS obtained the following vital signs: pulse 50, respiratory rate 16, blood pressure 96/49. It appears EMS obtained two EKGs, but unfortunately these were not saved in the medical record. The EMS crew was only BLS certified, so EKG interpretation is not within their scope of practice.
Such aggressive investigation was particularly warranted in this case because of symptoms compatible with ACS, as well as an equally frightening revelation of family history. Readers interested in a more robust discussion of STD vectors, and their implications in OMI, are encouraged to read this phenomenal post at the Smith ECG Blog.
Read More First10EM: Imaging for Renal Colic SGEM : SGEM XTRA: COME TOGETHER, RIGHT NOW – OVER RENAL COLIC References Chang, Helena, et al. Moore CL, Carpenter CR, Heilbrun ME, et al. Smith-Bindman R, Aubin C, Bailitz J, et al. PMID: 25229916 DOI: 10.1056/NEJMoa1404446 Westphalen AC, Hsia RY, Maselli JH, Wang R, Gonzales R.
link] Li Z, Krippendorff BF, Sharma S, Walz AC, Lavé T, Shah DK. Bush SP, Ruha AM, Seifert SA, et al. link] Kanaan NC, Ray J, Stewart M, et al. link] Full prescribing information. Crotalidae polyvalent immune fab (ovine). Published online January 2018. Accessed August 17, 2023. 2016;8(1):113-119. Published online November 2020.
Queen of Hearts now thinks that this one looks like posterior OMI, since the STD does appear worst in V3-4: None of this seems to have been understood by the EM doctor or the cardiologist who was consulted. In our opinion it should not be given in ACS unless you are committed to the cath lab. Hayakawa A, Tsukahara K, Miyagawa S, et al.
Personal take: While discussing this approach with many EM physicians whom we respect, one recurring critique was “We fought so hard to get the right to use paralytics in the ED, why would you want to go backwards.” References: Heffner AC et al. PMID: 23911630 Kim WY et al. PMID: 23911630 Kim WY et al. 2007): 748.
Anecdotally, had there been symptoms unequivocally consistent with ACS then one could justifiably make the case for a potential D1 occlusion. 4] Baranchuk, A, et al. Given such findings, serial ECG’s are prudent to consider, and carry significant impact moving forward, which has been demonstrated in previous posts. 2] Surawicz, B.
References: Ross RK, Kinlaw AC, Herzog MM, Funk MJ, Gerber JS. PMID: 27940800 Hersch AL, Gerber JS, Hicks LA, Pavia AT. PMID: 29356761 The post Fluoroquinolone Use In Children appeared first on Pediatric EM Morsels. However, Fluroquinolone resistance is increasing, so they should only be used if absolutely necessary!
A 60-something man presented by EMS with 5 hours of fairly typical sounding substernal chest pain. Here is the EMS ECG: Obviously massive diffuse subendocardial ischemia, with profound STD and STE in aVR Of course this pattern is most often seen from etoliogies other than ACS. Today’s Post by Dr.
EMS physicians report he was found in ventricular fibrillation. References Go AS, Mozaffarian D, Roger VL, et al. Larribau R, Deham H, Niquille M, et al. Margey R, Browne L, Murphy E, et al. Kudenchuk PJ, Brown SP, Daya M, et al. Spies DM, Kiekenap J, Rupp D, et al. Holmén J, Hollenberg J, Claesson A, et al.
A 44 year-old male with unknown past medical history came by emergency medical services (EMS) to the emergency department (ED) for an electrical injury and fall from a high voltage electrical pole. Per EMS, the patient was found at the bottom of a high voltage line with diffuse burns and amputation of his left forearm. 2023 Jul 17.
Paper: Mason JM, et al. This could have biased the results in favor of amiodarone as we’ve covered this before on REBEL EM before The IV amiodarone group required less additional HR control agents to control increased heart rate. These results were corroborated with other another study by Gritensko et al. Am J Emerg Med.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chest pain, weakness and nausea. En route, EMS administered aspirin 325mg by mouth, but withheld nitroglycerin due to initial hypotension. Answer below in the still shot. NEJM 362(9):779; March 4, 2009.
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al.
She did not receive any opioids (which would mask her pain without affecting any underlying ACS). Patel et al., Krucoff et al.) Patel et al. Krucoff et al. Schomig et al. Krucoff et al.) ) to disastrous consequences that may deteriorate before the patient can be rushed to the cath lab. Heart 1996.
Bourke Tillmann and Scott Weingart for their expertise on the EM Cases podcast that inspired this column. References Deshwal H, Sinha A, Mehta AC. Atchinson PRA, Hatton CJ, Roginski MA, et al. Ittrich H, Bockhorn M, Klose H, et al. Li H, Ding X, Zhai S, et al. Kathuria H, Hollingsworth HM, Vilvendhan R, et al.
Forestell B, Battaglia F, Sharif S, et al. Prekker ME, Bjorklund AR, Myers C, et al. O’Connell KJ, Sandler A, Dutta A, et al. O’Connell et al. O’Connell et al. Garabon JJW, Gunz AC, Ali A, Lim R. Garabon et al. Which way should we go? Crit Care Explor. 2023;5(2):e0857. Published 2023 Feb 17.
And according to a paper from Russotto et al. Of note, in the paper by Russotto et al., Dr. Jarvis of The EMS Lighthouse Project podcast also covers this paper in detail here: [link] ^^^ I highly recommend listening! Sackles et al. Heffner AC, Swords DS, Neale MN, Jones AE. De Jong A, Molinari N, Terzi, et al.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content