This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
That discussion can be deferred until the patient is stable, the risk of such an event is mitigated, and other medications can be given for their withdrawal symptoms and pain. Multimodal medication options for fentanyl-xylazine withdrawal management in London et al. DOI: Papudesi BN, Malayala SV, Regina AC. 2024 study [16].
Studies such as those by Moise et al 14 and Ellis et al 39 have shown that the relative risk of developing an acute myocardial infarction in the territory supplied by an artery with a 70%. Furthermore, if this occurs at all, it is a rare event. years, with the interval as long as 12 or 18 years in some studies.
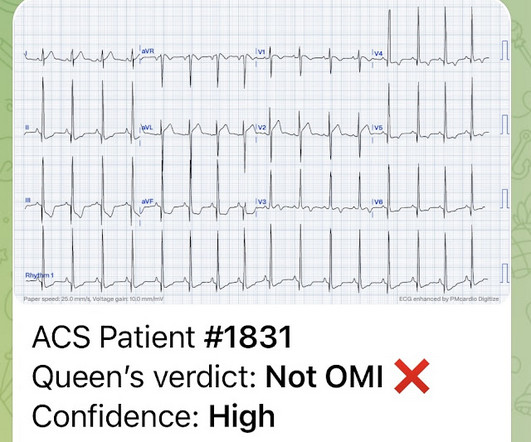
What Your Gut Says: The patient has a tachydysrhythmia which may be the presentation of acute coronary syndrome (ACS) even though the patient has no ischemic symptoms. There are other reasons aside from ACO for troponin elevations: Type 1: MI due to a spontaneous coronary atherosclerotic event. Send the troponin just to make sure.
Date: June 30th, 2022 Reference: McGinnis et al. Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Date: June 30th, 2022 Reference: McGinnis et al. Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Reference: McGinnis et al.
Myth 1 Absence of Classic Chest Pain obviates the need for ACS work up The absence of chest pain in no way excludes the diagnosis of ACS. Around 33-50% of the patients with ACS present to the hospital without chest pain. References: Canto JG, Shlipak MG, Rogers WJ, et al. Dorsch MF, Lawrence RA, Sapsford RJ, et al.
VS abnormalities can drive this as well Strongly consider reversal of AC (this will typically come after control) Stopping the Bleeding PPE: these things bleed like stink. EMRAP HD: Epistaxis Posterior Pack References Cassisi NJ et al. PMID: 5569677 Zeyyan E et al. PMID: 20938948 Loftus BC et al.
Angiogram No obstructive epicardial coronary artery disease Cannot exclude non-ACS causes of troponin elevation including coronary vasospasm, stress cardiomyopathy, microvascular disease, etc. Even in patients whose moderate stenosis undergoes thrombosis, most angiograms show greater than 50% stenosis after the event. Lindahl et al.
Click here for Direct Download of the Podcast Paper: Aykan AC et al. References: Jaff MR et al. PMID: 21422387 Wan S et al. PMID: 15262836 Sharifi M et al. PMID: 27422214 Wang C et al. PMID: 19741062 Kucher N et al. PMID: 24226805 Piazza G et al. PMID: 26315743 Tapson VF et al.
Myth #1: Musculoskeletal Adverse Events (MAE) This concern is likely the most common reason fluoroquinolones are rarely used in children. Musculoskeletal Adverse Events include: Articular cartilage damage causing arthralgias or arthritis , Tendonitis , and Tendon rupture. Which is a risk of 1 event for 62.5 Binz 2015).
Thus, these troponins are very concerning for ACS, and subsequent ones will probably be diagnostic of acute MI. Heitner et al. For this test it is VERY low (very good) at 4% at the 99th percentile -- 26 ng/L, but it will not be so good at a level of 9 ng/L. The troponin is trapped in the myocardium that is not being perfused.
Because there was proven thrombus (ACS) but the troponin never went above the 99% reference range (and therefore cannot be called MI -- definition of MI requires rise and/or fall of troponin with at least one value above the 99% reference range), this is UNSTABLE ANGINA with ST Elevation. This is not the case.
3) RV Failure leads to hypotension but NOT pulmonary edema (unlike LV failure) 4) Repeat ECGs, right sided ECG and bedside echo may be helpful in making a diagnosis of ACS. As a result — the onset of any acute event that may have occurred is uncertain. 21, 2017 ).
The trade off to using FI for these challenging airways is the consideration of an aspiration event, the initial indication for RSI. First pass success (FPS) is key as increased attempts correlate to increased desaturation (>10%) events (~10% on first attempt, ~30% on second attempt, ~60% for 4+ attempts) (15).
In our opinion it should not be given in ACS unless you are committed to the cath lab. Learning Point: Any NSTEMI patient with active ongoing ACS symptoms refractory to medical management is supposed to go to the cath lab within 2 hours if available, per all guidelines in world, regardless of ECG findings. Am J Emerg Med.
Anecdotally, had there been symptoms unequivocally consistent with ACS then one could justifiably make the case for a potential D1 occlusion. Whether this represents a potential acute cardiac event would depend on the history, comparison with prior tracings and serial tracings. 4] Baranchuk, A, et al. 2] Surawicz, B.
Lemkes et al. No wall motion abnormality This shows that significant ACS can have ZERO WMA!! Impression: In a patient with new symptoms — early repolarization is a diagnosis of exclusion to be made only after you have ruled out the possibility of an acute event. The Proximal LAD thrombus lysed or partially lysed, restoring flow.
But because the patient had no chest pain or shortness of breath, it was not deemed to be from ACS. They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS. Dialysis patients have a high rate of ACS without chest pain and high rate of delayed diagnosis and delayed reperfusion 2.
There were zero patients in this study with a "normal" ECG who had any kind of ACS! Deutch et al. This defies all previous data on acute MI which would show that even undetectable troponins do not have a 100% negative predictive value. So this study is actually worthless. West J Emerg Med 2024).
SCAD isn’t rare, especially in women Historically SCAD had been identified in 22% of ACS cases in women. Pregnancy is not a common cause of SCAD When ACS occurs in the peripartum period, SCAD is responsible in 43% of cases. A study by Hassan et al. A study by Hassan et al. Lobo et al. The SCAD cases in Lobo et al.
ED treatment should focus on airway, breathing, and circulation with consideration for cervical spine protection depending on the circumstances surrounding the event. References Webb AC, Wheeler A, Ricci A, et al. Pellegrino F, Raffaldi I, Rossi R, et al. Chotai PN, Manning L, Eithun B, et al. South Med J.
Datz, Christian, et al. ACS omega , 7 (24), pp.20441-20456. Hodgskiss, Malcolm SW, et al. Moalem, Sharon, et al. Olejarz, Jason, et al. “The Great Oxygenation Event as a consequence of ecological dynamics modulated by planetary change.” Wade, Jon, et al. 1991): 28-31. Pietrangelo, A.,
And according to a paper from Russotto et al. titled “Intubation Practices and Adverse Peri-intubation Events in Critically Ill Patients from 29 Countries,” at least one major critical event occurred after intubation in 45.2% Of note, in the paper by Russotto et al., are at high risk.
The fire department, who operate at an EMT level in this municipality, arrived before us and administered 324 mg of baby aspirin to the patient due to concern for ACS. Takotsubo is a sudden event, not one with crescendo angina. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al. Lindahl et al.
1 The American College of Surgeons’ (ACS) Trauma Quality Improvement Program (TQIP) Massive Transfusion in Trauma Guidelines leave a good amount of flexibility for hospitals regarding transfusion protocols, focusing more on systems-level aspects of designing and implementing MTPs.2,3 Holcomb JB, Tilley BC, Baraniuk S, et al.
It is also true that anterior and inferior T-wave inversion could be consistent with reperfusion of a type III wraparound LAD occlusion, despite the fact that Kosuge et al showed that T-wave inversion in lead III is much more likely to be PE than ACS if your differential contains nothing else. Stein et al. Kosuge et al.
I did not think it was due to ACS, but we ordered an ED ECG immediately: What do you think? But in this case the clinical scenario is not right for acute ACS with OMI, and there is very high voltage, and the patient is very young, (though beware of young patients , even 29 year olds!! There is profound "inferior" ST Depression.
Forestell B, Battaglia F, Sharif S, et al. Results of this study showed that the use of low-dose insulin infusion led to similar clinical outcomes and fewer adverse events compared to the standard-dose insulin infusion. units/kg/hr ) is as efficacious as standard-dose, with fewer adverse events. O’Connell et al.
The patient would not have been diagnosed with acute coronary syndrome and would not have had an angiogram, would have been discharged (or perhaps had a stress test, which would be negative), and would be at great risk of another event, possibly resulting in death or heart failure. Thelin et al. Mokhtari et al.
Although this is considered a "STEMI equivalent" and the ACC/AHA guidelines even approve of thrombolytics for ACS with this ECG, the usual criteria used to alert the cath lab team of an inbound Code STEMI are not met by this ECG. For instance: sepsis, bleeding, dehydration, hypoxia, and mild ACS. NEJM 362(9):779; March 4, 2009.
She did not receive any opioids (which would mask her pain without affecting any underlying ACS). Patel et al., Krucoff et al.) Patel et al. Krucoff et al. Schomig et al. Krucoff et al.) ) to disastrous consequences that may deteriorate before the patient can be rushed to the cath lab. Heart 1996.
Considering hyperacute T-waves have been accepted as STEMI equivalents, it is possible that pseudonormalization could gain more recognition as an indicator of ACS. Sequence of events in angina at rest: Primary reduction in coronary flow. References Noble RJ, Rothbaum DA, Knoebel SB, McHenry PL, Anderson GJ. Arch Intern Med.
Sodhi M, Rezaeianzadeh R, Kezouh A, et al. Risk of gastrointestinal adverse events associated with glucagon-like peptide-1 receptor agonists for weight loss. Ahmann AJ, Capehorn M, Charpentier G, et al. ACS chemical neuroscience molecule spotlight on Contrave. ACS Chem Neurosci. Bansal AB, Al Khalili Y.
He had no symptoms of ACS. His HEAR score (before troponin resulted) was documented at 3, with documentation stating "low suspicion for ACS." A troponin this high in a patient with no known chronic troponin elevation, and active acute ACS symptoms, has a very high likelihood of type 1 ACS regardless of the ECG.
It was shown to me with worry for ischemic ST elevation, which is certainly possible from severe CO toxicity, or concomitant ACS. Yelken B et al. Intravascular Neutrophil Activation Due to Carbon Monoxide Poisoning What do you think of this ECG?
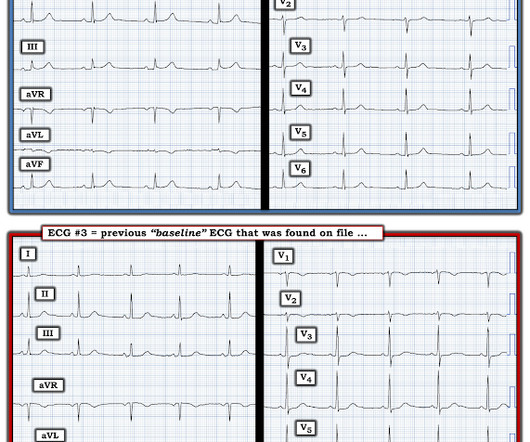
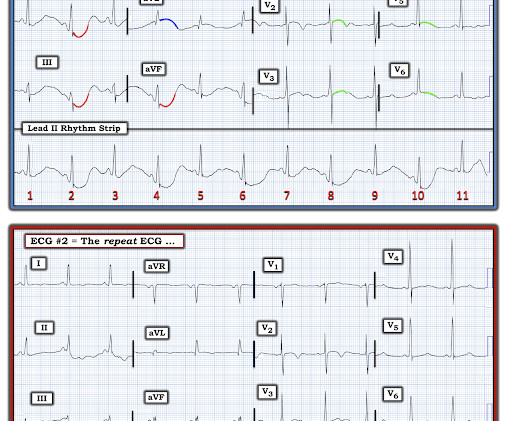
MY Impression of ECG #2: Keeping in mind that the patient in today's case presented with chest pain — the nonspecific ST-T wave flattening in multiple leads, with T wave inversion in lead V2 could be ischemic — albeit clearly not suggestive of an acute event! The January 30, 2018 post — for arterial pulsation artifact.
The ECG is diagnostic for acute transmural infarction of the anterior and lateral walls, with LAD OMI being the most likely cause (which has various potential etiologies for the actual cause of the acute coronary artery occlusion, the most common of which is of course type 1 ACS, plaque rupture with thrombotic occlusion).
3–8 Shi et al. Sandoval Y, Smith SW, Sexter A, et al. Shi S, Qin M, Shen B, et al. Guo T, Fan Y, Chen M, et al. Lala A, Johnson KW, Russak AJ, et al. He XW, Lai JS, Cheng J, et al. of Cardiology AC, Others. Sandoval Y, Thordsen SE, Smith SW, et al. Bangalore S, Sharma A, Slotwiner A, et al.
The more additional leads that we can identify in ECG #1 that show ST-T wave abnormalities — the greater the likelihood that our suspicion for an acute cardiac event ( based on this history + the ST-T wave appearance in leads V2 and V3 ) is correct: The ST-T wave in neighboring lead V 1 of ECG #1 is abnormal. It is not normal to see ≥1.5
Here is a Previous ECG for comparison: Baseline LVH Only minimal ST depression Diffuse ST depression with ST Elevation in aVR Knotts et al. found that such ECG findings only represented left main ACS in 14% of such ECGs: Only 23% of patients with the aVR STE pattern had any LM disease (fewer if defined as 50% stenosis).
I C Glucose-lowering therapy should be considered in ACS patients with glucose levels >10 mmol/L (>180 mg/dL), while episodes of hypoglycaemia (defined as glucose levels <_3.9 I C In patients on metformin and/or SGLT2 inhibitors, renal function should be monitored for at least 3 days after angiography.
Compare this with the Panickar et al. Fortunately, Lee et al. Lee B, Turner S, Borland M, Csonka P, Grigg J, Guilbert TW, et al. Whilst the incidence of adverse events was low in this meta-analysis, this reflects adverse event reporting in RCTs rather than reality. Future of Pre-School Wheeze Whilst Lee et al.
There were trends toward larger infarct size with delayed angiography, both by cMR and integral high-sensitivity troponin concentration, as well as toward higher rate of major adverse cardiovascular events (MACE) (8.5 Kontos et al. Welsh et al. Busk et al. Eur Heart J 2009 4 Lemkes et al. Int J Cardiol 2016 3.
6 Prolonged down time from falls, usually in the elderly Incidence is difficult to ascertain due to broad definition and that events that cause crush injuries are rather rare. Oda J, Tanaka H, Yoshioka T, et al. Tanaka H, Oda J, Iwai A, et al. Goodman AD, Got CJ, Weiss AC. Chen CY, Lin YR, Zhao LL, et al.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content