This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
We have certainly seen patients who have pain which is controlled and still have psychomotor agitation and sympathetic activation, leading some to require ICU admission for dexmedetomidine and/or ketamine infusion. Multimodal medication options for fentanyl-xylazine withdrawal management in London et al. mg IVP Tizanidine 4 mg PO 0.15
VS abnormalities can drive this as well Strongly consider reversal of AC (this will typically come after control) Stopping the Bleeding PPE: these things bleed like stink. The idea behind abx is to prevent things like AOM and TSS but neither should be much of an issue with short term placement ICU Admission?
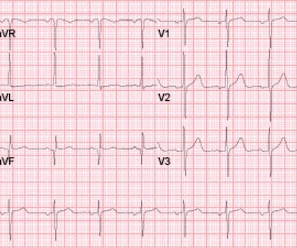
The patient was upgraded to the ICU for closer monitoring. In fact, Kosuge et al. Stein et al. This is a paper worth reading : Marchik et al. Kosuge et al. showed that , when T-waves are inverted in precordial leads, if they are also inverted in lead III and V1, then pulmonary embolism is far more likely than ACS.
Article: Vaeli Zadeh A, Wong A, Crawford AC, Collado E, Larned JM. Secondary Outcomes: Delayed hypotension, increased ICU stay, and other relevant outcomes. Uchel et al’s contribution (21% weight) indicates that ≥30cc/kg IVF is linked to 2.5 Outcomes: Primary Outcome: In-hospital mortality. 2.89, p = 0.01.
100% seems too good to be true Morello et al., Clin Exp Allergy. 2024 Oct 9. doi: 10.1111/cea.14565. Epub ahead of print. PMID: 39383344 Profundus Trial – Can we actually exclude acute aortic syndromes with this protocol? Diagnosis of acute aortic syndromes with ultrasound and D-dimer: the PROFUNDUS study. Emerg Med J. Epub 2018 Oct 25.
Removed from cooling at 102 and admitted to ICU. 2016 study published in American Journal of Emergency Medicine , “ Urinary obstruction is an important complicating factor in patients with septic shock due to urinary infection ” by Reyner et al. Reference: Reyner K, Heffner AC, Karvetski CH. Temperature starts to decrease.
The NIHSS cutoff that predicts outcomes is 4 points higher in AC compared with PC infarctions. All patients who receive thrombolytics for ischemic stroke should be admitted to a neurosurgical, neurologic, or medical ICU for management and monitoring, as this is shown to decrease mortality and length of stay. Arch Neurol.
Type 1 is the acute deterioration in kidney function seen in cardiogenic shock from ACS. It is important to realise that a referral to ICU for refractory cardiorenal syndrome may simply be a sign that the patient is reaching end of life. Type 1 is the acute deterioration in kidney function seen in cardiogenic shock from ACS.
Despite the risk of hypotension and bradycardia, propofol has been shown in the ICU setting to be a safe and effective monotherapy intubation agent for hemodynamically unstable patients (19). References: Heffner AC et al. PMID: 23911630 Kim WY et al. PMID: 23911630 Kim WY et al. PMID: 25402500 Forsythe SM et al.
Taking a different approach than the authors of the AHRQ report, Auerbach et al used a “look back” approach to perform both qualitative and quantitative evaluations of the types and frequencies of errors occurring in hospital settings. After developing encephalopathy and hypoxemic respiratory failure, the patient was transferred to the ICU.
It is also true that anterior and inferior T-wave inversion could be consistent with reperfusion of a type III wraparound LAD occlusion, despite the fact that Kosuge et al showed that T-wave inversion in lead III is much more likely to be PE than ACS if your differential contains nothing else. Stein et al. Kosuge et al.
She did not receive any opioids (which would mask her pain without affecting any underlying ACS). If for some reason the angiogram is delayed, they should receive maximal medical therapy in an ICU setting with continuous 12-lead ST segment monitoring under the close attention of a practitioner with advanced ECG interpretation training.
They found NO difference in drain failure rates ( 11% pigtail vs 13% chest tube P=0.74), total daily volume drained or length of ICU stay between groups. Kulvatunyou N, Bauman ZM, Zein Edine SB, de Moya M, Krause C, Mukherjee K, Gries L, Tang AL, Joseph B, Rhee P. Laan DV, Vu TD, Thiels CA et al. Trauma Surg Acute Care Open.
1 The American College of Surgeons’ (ACS) Trauma Quality Improvement Program (TQIP) Massive Transfusion in Trauma Guidelines leave a good amount of flexibility for hospitals regarding transfusion protocols, focusing more on systems-level aspects of designing and implementing MTPs.2,3 Holcomb JB, Tilley BC, Baraniuk S, et al.
Below follows a drug manual for use in the CCU (coronary care unit), ICU (intensive care unit) or ER (emergency room). References Overgaard, Dzavik et al. Jentzer et al. Müllner M, Urbanek B, Havel C, et al. Lherm T, Troché G, Rossignol M, et al. Gattinoni L, Brazzi L, Pelosi P, et al. Circulation 2011.
2 Amiodarone is commonly known for its anti-arrhythmic properties and a commonly used agent in the Intensive Care Unit (ICU). Paper: Mason JM, et al. These results were corroborated with other another study by Gritensko et al. Sepsis, hyperthyroidism, dehydration, heart failure, ACS, etc). References Mason JM, et al.
Paper: Nassal MMJ, et al. An example using a real case I had while on call in the ICU: A 61-year-old female had a post-induction arrest on the wards/hospital telemetry floor after being intubated for airway protection. REFERENCES: Nassal MMJ, et al. PMID: 34968531 Rittenberger JC, et al. PMID: 21756969 Coppler PJ, et al.
Hematologic Management Takeaway : They recommend a transfusion threshold < 9 g/dL in those with ACS, but several studies (MINT trial) and guidelines suggest 8 g/dL can be used. Digestive Management Takeaway: Start enteral feeds when the patient gets to the ICU. Administer VTE prophylaxis in the first 48 hours, preferably LMWH.
References Deshwal H, Sinha A, Mehta AC. Atchinson PRA, Hatton CJ, Roginski MA, et al. Ittrich H, Bockhorn M, Klose H, et al. Li H, Ding X, Zhai S, et al. Kathuria H, Hollingsworth HM, Vilvendhan R, et al. Fekri MS, Hashemi-Bajgani SM, Shafahi A, et al. Wand O, Guber E, Guber A, et al. Am J Emerg Med.
Lupu L, et al. Smith comment: We have shown that use of opiates is associated with worse outcomes in ACS: Bracey, A. The facility was not pressed to activate emergent transfer for PCI since the pain was improving and suggested we optimize pain control and admit to the Cardiac ICU. mg/dL, K 3.5 OMI is not just an ECG diagnosis.
Forestell B, Battaglia F, Sharif S, et al. Prekker ME, Bjorklund AR, Myers C, et al. O’Connell KJ, Sandler A, Dutta A, et al. O’Connell et al. O’Connell et al. Garabon JJW, Gunz AC, Ali A, Lim R. Garabon et al. Which way should we go? Crit Care Explor. 2023;5(2):e0857. Published 2023 Feb 17.
I took part in her ICU care and she was extubated and stable to transfer to a stepdown unit after a few days. Patients like her are the reason we are advocating for a change in the ACS paradigm from STEMI to OMI. Her repeat ECHO showed an improving EF of 37%. Note that this is completely different from 'terminal QRS distortion'.
10 Although this is not the same pathophysiology seen in ACS from an acute plaque rupture leading to coronary artery occlusion, patients can have relatively abrupt coronary ischemia causing ACS due to acute, concentric vessel narrowing. 3 Many will experience vague, nonspecific symptoms such as weakness or fatigue.
Oda J, Tanaka H, Yoshioka T, et al. Tanaka H, Oda J, Iwai A, et al. Goodman AD, Got CJ, Weiss AC. Chen CY, Lin YR, Zhao LL, et al. Wald R, Quinn RR, Luo J, et al. Somagutta MR, Pagad S, Sridharan S, et al. Crush Injuries with Impairment of Renal Function. 1941;1(4185):427-432. Am J Emerg Med. Critical Care.
In this situation, an ABG should be obtained periodically for correlation, though this is more relevant for the intensive care unit (ICU) setting than in routine ED care (5, 9). References/Further Reading (1) Byrne AL, Bennett M, Chatterji R, Symons R, Pace NL, Thomas PS. 11) Webb RK, Ralston AC, Runciman WB. PMID: 11685301. (10)
Alkindi S, Al-Busaidi I, Al-Salami B, Raniga S, Pathare A, Ballas SK. Alghamdi FA, Al-Kasim F, Alshhada F, Ghareeb E, Azmet FR, Almudaibigh A, Baitalmal L, Alnawfal B, Alluqmani R. Chinawa JM, Ubesie AC, Chukwu BF, Ikefuna AN, Emodi IJ. C or 100.4 mg/kg, max 4 mg per dose q20-30min) or hydromorphone (0.01-0.02
Disposition is often admission to an intensive care unit (ICU) setting. Further management and resuscitation were required, and she had a lengthy ICU stay of 21 days until she was extubated. References: Boostani R, Mellat A, Afshari R, et al: Delayed polyneuropathy in farm sprayers due to chronic low dose pesticide exposure.
Opioids do not cause ACS but they can exacerbate hypoxia in patients with ACS. Older children and adults usually present with ACS 2-3 days after hospitalisation due to pulmonary infarction (in situ sickling), hypoventilation due to rib infarction (which may be exacerbated by recent narcotic administration) or fat embolism.
To assess the clinical impact and relevance of these concerns, Alwang et al. Paper: Alwang AK, Law AC, Klings ES, Cohen RT, Bosch NA. PMID: 28423290 Kidwell K, Albo C, Pope M, et al. PMID: 24066745 Self WH, Semler MW, Wanderer JP, et al. PMID: 29485926 Semler MW, Self WH, Wanderer JP, et al. JAMA Intern Med.
84 All patients with severe malaria need inpatient admission, ideally to the intensive care unit (ICU). 57 Adapted from: Long B, MacDonald A, Liang SY, et al. link] Rother B, Pierre G, Lombardo D, et al. link] Hummell AC, Cummings M. link] Franco JR, Cecchi G, Priotto G, et al. 57 Table 2. 2024;77:7-16.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
































Let's personalize your content