This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Alternatively, one can cut the 2 mg Suboxone (buprenorphine + naloxone combination) strips into 4 pieces after waiting for a longer washout period (72-96 hours of abstinence from non-medical opioids) before starting the induction. Multimodal medication options for fentanyl-xylazine withdrawal management in London et al. 2023 [book].
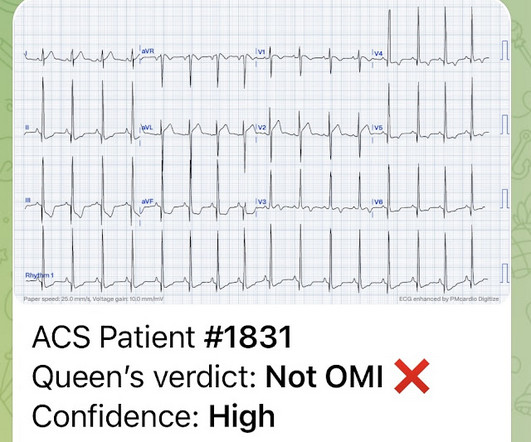
This 29 year old African American patient was found down, unconscious, not breathing and was given 2 mg of intranasal naloxone by a bystander. I did not think it was due to ACS, but we ordered an ED ECG immediately: What do you think? He then received bag-valve-mask ventilations for several minutes until he became responsive.
A 33-year-old male with a history of drug use presented to the emergency department (ED) for extreme agitation after receiving two doses of 2 mg naloxone by EMS for respiratory depression. Gummin DD, Mowry JB, Beuhler MC, et al. Todd DA, Kellogg JJ, Wallace ED, et al. Obeng S, Kamble SH, Reeves ME, et al. 2022;23(1):4-9.
mg q20-30 min per dose) PRN naloxone in case of respiratory depression Some patients have SCD crises pain plan for reference Antimicrobials 11 Ceftriaxone + azithromycin if penicillin allergy for both children and adults. Alkindi S, Al-Busaidi I, Al-Salami B, Raniga S, Pathare A, Ballas SK. C or 100.4 mg/kg, max 0.4 C or 100.4
Opioids do not cause ACS but they can exacerbate hypoxia in patients with ACS. Naloxone (opioid antidote) should be available in ED in case of severe respiratory depression. The treatment for ACS is mainly supportive: Oxygen : supplemental oxygen should be given only when the patient is hypoxic (saturation of oxygen < 94%).
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











Let's personalize your content